Department of Anaesthesiology, Intensive Care, Emergency and Pain Medicine, University Hospital Wuerzburg, Wuerzburg, Germany.
Department of Infectious Diseases and Respiratory Medicine, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany.
Cochrane Database Syst Rev. 2021 Jul 28;7(7):CD015017. doi: 10.1002/14651858.CD015017.pub2.
Ivermectin, an antiparasitic agent used to treat parasitic infestations, inhibits the replication of viruses in vitro. The molecular hypothesis of ivermectin's antiviral mode of action suggests an inhibitory effect on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) replication in the early stages of infection. Currently, evidence on efficacy and safety of ivermectin for prevention of SARS-CoV-2 infection and COVID-19 treatment is conflicting.
To assess the efficacy and safety of ivermectin compared to no treatment, standard of care, placebo, or any other proven intervention for people with COVID-19 receiving treatment as inpatients or outpatients, and for prevention of an infection with SARS-CoV-2 (postexposure prophylaxis).
We searched the Cochrane COVID-19 Study Register, Web of Science (Emerging Citation Index and Science Citation Index), medRxiv, and Research Square, identifying completed and ongoing studies without language restrictions to 26 May 2021.
We included randomized controlled trials (RCTs) comparing ivermectin to no treatment, standard of care, placebo, or another proven intervention for treatment of people with confirmed COVID-19 diagnosis, irrespective of disease severity, treated in inpatient or outpatient settings, and for prevention of SARS-CoV-2 infection. Co-interventions had to be the same in both study arms. We excluded studies comparing ivermectin to other pharmacological interventions with unproven efficacy.
We assessed RCTs for bias, using the Cochrane risk of bias 2 tool. The primary analysis excluded studies with high risk of bias. We used GRADE to rate the certainty of evidence for the following outcomes 1. to treat inpatients with moderate-to-severe COVID-19: mortality, clinical worsening or improvement, adverse events, quality of life, duration of hospitalization, and viral clearance; 2. to treat outpatients with mild COVID-19: mortality, clinical worsening or improvement, admission to hospital, adverse events, quality of life, and viral clearance; (3) to prevent SARS-CoV-2 infection: SARS-CoV-2 infection, development of COVID-19 symptoms, adverse events, mortality, admission to hospital, and quality of life.
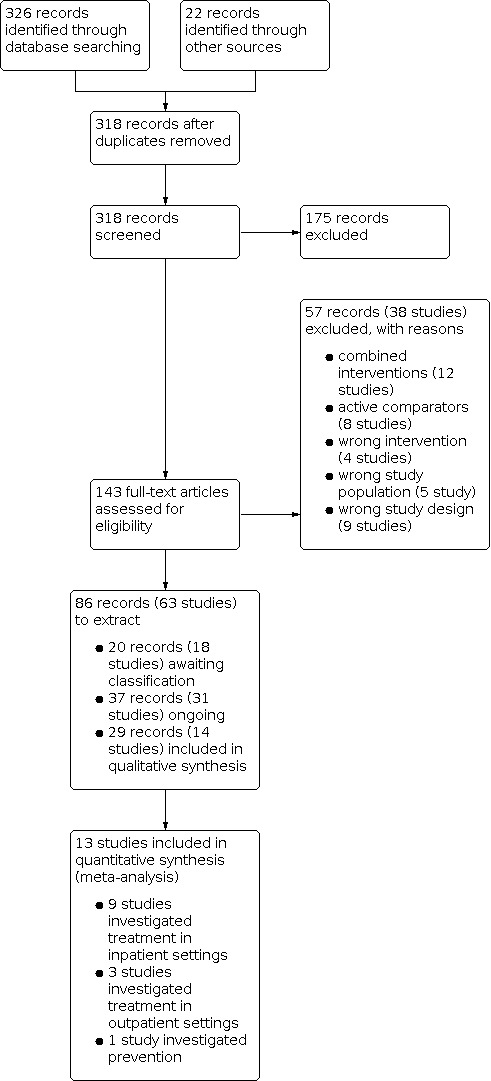
We found 14 studies with 1678 participants investigating ivermectin compared to no treatment, placebo, or standard of care. No study compared ivermectin to an intervention with proven efficacy. There were nine studies treating participants with moderate COVID-19 in inpatient settings and four treating mild COVID-19 cases in outpatient settings. One study investigated ivermectin for prevention of SARS-CoV-2 infection. Eight studies had an open-label design, six were double-blind and placebo-controlled. Of the 41 study results contributed by included studies, about one third were at overall high risk of bias. Ivermectin doses and treatment duration varied among included studies. We identified 31 ongoing and 18 studies awaiting classification until publication of results or clarification of inconsistencies. Ivermectin compared to placebo or standard of care for inpatient COVID-19 treatment We are uncertain whether ivermectin compared to placebo or standard of care reduces or increases mortality (risk ratio (RR) 0.60, 95% confidence interval (CI) 0.14 to 2.51; 2 studies, 185 participants; very low-certainty evidence) and clinical worsening up to day 28 assessed as need for invasive mechanical ventilation (IMV) (RR 0.55, 95% CI 0.11 to 2.59; 2 studies, 185 participants; very low-certainty evidence) or need for supplemental oxygen (0 participants required supplemental oxygen; 1 study, 45 participants; very low-certainty evidence), adverse events within 28 days (RR 1.21, 95% CI 0.50 to 2.97; 1 study, 152 participants; very low-certainty evidence), and viral clearance at day seven (RR 1.82, 95% CI 0.51 to 6.48; 2 studies, 159 participants; very low-certainty evidence). Ivermectin may have little or no effect compared to placebo or standard of care on clinical improvement up to 28 days (RR 1.03, 95% CI 0.78 to 1.35; 1 study; 73 participants; low-certainty evidence) and duration of hospitalization (mean difference (MD) -0.10 days, 95% CI -2.43 to 2.23; 1 study; 45 participants; low-certainty evidence). No study reported quality of life up to 28 days. Ivermectin compared to placebo or standard of care for outpatient COVID-19 treatment We are uncertain whether ivermectin compared to placebo or standard of care reduces or increases mortality up to 28 days (RR 0.33, 95% CI 0.01 to 8.05; 2 studies, 422 participants; very low-certainty evidence) and clinical worsening up to 14 days assessed as need for IMV (RR 2.97, 95% CI 0.12 to 72.47; 1 study, 398 participants; very low-certainty evidence) or non-IMV or high flow oxygen requirement (0 participants required non-IMV or high flow; 1 study, 398 participants; very low-certainty evidence). We are uncertain whether ivermectin compared to placebo reduces or increases viral clearance at seven days (RR 3.00, 95% CI 0.13 to 67.06; 1 study, 24 participants; low-certainty evidence). Ivermectin may have little or no effect compared to placebo or standard of care on the number of participants with symptoms resolved up to 14 days (RR 1.04, 95% CI 0.89 to 1.21; 1 study, 398 participants; low-certainty evidence) and adverse events within 28 days (RR 0.95, 95% CI 0.86 to 1.05; 2 studies, 422 participants; low-certainty evidence). None of the studies reporting duration of symptoms were eligible for primary analysis. No study reported hospital admission or quality of life up to 14 days. Ivermectin compared to no treatment for prevention of SARS-CoV-2 infection We found one study. Mortality up to 28 days was the only outcome eligible for primary analysis. We are uncertain whether ivermectin reduces or increases mortality compared to no treatment (0 participants died; 1 study, 304 participants; very low-certainty evidence). The study reported results for development of COVID-19 symptoms and adverse events up to 14 days that were included in a secondary analysis due to high risk of bias. No study reported SARS-CoV-2 infection, hospital admission, and quality of life up to 14 days.
AUTHORS' CONCLUSIONS: Based on the current very low- to low-certainty evidence, we are uncertain about the efficacy and safety of ivermectin used to treat or prevent COVID-19. The completed studies are small and few are considered high quality. Several studies are underway that may produce clearer answers in review updates. Overall, the reliable evidence available does not support the use ivermectin for treatment or prevention of COVID-19 outside of well-designed randomized trials.
伊维菌素是一种用于治疗寄生虫感染的驱虫药,可抑制病毒在体外的复制。伊维菌素抗病毒作用的分子假说表明,它可能抑制严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染早期的复制。目前,关于伊维菌素在 COVID-19 治疗或预防中的疗效和安全性的证据相互矛盾。
评估伊维菌素与无治疗、标准护理、安慰剂或任何其他已证实的干预措施相比,在治疗门诊或住院患者的 COVID-19 以及预防 SARS-CoV-2 感染(暴露后预防)方面的疗效和安全性。
我们检索了 Cochrane COVID-19 研究注册库、Web of Science(新兴引文索引和科学引文索引)、medRxiv 和 Research Square,确定了截至 2021 年 5 月 26 日已完成和正在进行的研究,且无语言限制。
我们纳入了比较伊维菌素与无治疗、标准护理、安慰剂或其他已证实的干预措施治疗确诊 COVID-19 患者的随机对照试验(RCT),无论疾病严重程度如何,均在门诊或住院环境中进行治疗,以及预防 SARS-CoV-2 感染。联合治疗必须在研究组中相同。我们排除了比较伊维菌素与其他疗效未经证实的药物干预的研究。
我们使用 Cochrane 偏倚风险 2 工具评估了 RCT 的偏倚。主要分析排除了高偏倚风险的研究。我们使用 GRADE 来评估以下结局的证据确定性:1. 治疗中重度 COVID-19 的住院患者:死亡率、临床改善或恶化、不良事件、生活质量、住院时间和病毒清除率;2. 治疗轻度 COVID-19 的门诊患者:死亡率、临床改善或恶化、住院、不良事件、生活质量和病毒清除率;3. 预防 SARS-CoV-2 感染:SARS-CoV-2 感染、COVID-19 症状发展、不良事件、死亡率、住院和生活质量。
我们发现了 14 项研究,涉及 1678 名参与者,研究了伊维菌素与无治疗、安慰剂或标准护理的比较。没有研究比较伊维菌素与已证实有效的干预措施。有 9 项研究治疗中度 COVID-19 的住院患者,4 项研究治疗轻度 COVID-19 的门诊患者。一项研究调查了伊维菌素预防 SARS-CoV-2 感染。8 项研究为开放标签设计,6 项为双盲和安慰剂对照。纳入研究的 41 项研究结果中,约有三分之一的研究存在总体高偏倚风险。伊维菌素的剂量和治疗持续时间在纳入的研究中有所不同。我们发现 31 项正在进行的研究和 18 项研究有待分类,直到发表结果或澄清不一致之处。
伊维菌素与安慰剂或标准护理比较治疗住院 COVID-19 患者:我们不确定伊维菌素与安慰剂或标准护理相比是否能降低或增加死亡率(风险比(RR)0.60,95%置信区间(CI)0.14 至 2.51;2 项研究,185 名参与者;非常低确定性证据)和临床恶化至第 28 天(需要有创机械通气(IMV)评估为需要(RR 0.55,95%CI 0.11 至 2.59;2 项研究,185 名参与者;非常低确定性证据)或需要补充氧气(RR 0.00,1 项研究,45 名参与者;非常低确定性证据),28 天内的不良事件(RR 1.21,95%CI 0.50 至 2.97;1 项研究,152 名参与者;非常低确定性证据),以及第 7 天的病毒清除率(RR 1.82,95%CI 0.51 至 6.48;2 项研究,159 名参与者;非常低确定性证据)。伊维菌素与安慰剂或标准护理相比,28 天内的临床改善(RR 1.03,95%CI 0.78 至 1.35;1 项研究;73 名参与者;低确定性证据)和住院时间(平均差值(MD)-0.10 天,95%CI-2.43 至 2.23;1 项研究;45 名参与者;低确定性证据)可能几乎没有或没有影响。没有研究报告 28 天的生活质量。
伊维菌素与安慰剂或标准护理比较治疗门诊 COVID-19 患者:我们不确定伊维菌素与安慰剂或标准护理相比是否能降低或增加死亡率至第 28 天(RR 0.33,95%CI 0.01 至 8.05;2 项研究,422 名参与者;非常低确定性证据)和临床恶化至第 14 天(需要有创机械通气(RR 2.97,95%CI 0.12 至 72.47;1 项研究,398 名参与者;非常低确定性证据)或非有创机械通气或高流量氧需求(RR 0.00,1 项研究,398 名参与者;非常低确定性证据)。我们不确定伊维菌素与安慰剂相比是否能降低或增加第 7 天的病毒清除率(RR 3.00,95%CI 0.13 至 67.06;1 项研究,24 名参与者;低确定性证据)。伊维菌素与安慰剂或标准护理相比,28 天内症状缓解的参与者数量(RR 1.04,95%CI 0.89 至 1.21;1 项研究,398 名参与者;低确定性证据)和不良事件(RR 0.95,95%CI 0.86 至 1.05;2 项研究,422 名参与者;低确定性证据)可能几乎没有或没有影响。没有报告持续症状的研究符合主要分析的资格。没有研究报告 14 天的住院率或生活质量。
伊维菌素与无治疗比较预防 SARS-CoV-2 感染:我们发现了一项研究。第 28 天的死亡率是唯一符合主要分析条件的结局。我们不确定伊维菌素是否降低或增加死亡率(0 名参与者死亡;1 项研究,304 名参与者;非常低确定性证据)。该研究报告了第 14 天发展为 COVID-19 症状和不良事件的结果,由于偏倚风险高,被纳入次要分析。没有研究报告 SARS-CoV-2 感染、住院和第 14 天的生活质量。
根据目前非常低至低确定性证据,我们对伊维菌素治疗或预防 COVID-19 的疗效和安全性不确定。已完成的研究规模较小,且很少有研究被认为质量较高。有几项研究正在进行中,可能会在综述更新中产生更清晰的答案。总体而言,现有的可靠证据不支持伊维菌素在 COVID-19 治疗或预防之外的良好设计的随机试验中使用。