Caccialanza Riccardo, Formisano Elena, Klersy Catherine, Ferretti Virginia, Ferrari Alessandra, Demontis Stefania, Mascheroni Annalisa, Masi Sara, Crotti Silvia, Lobascio Federica, Cerutti Nadia, Orlandoni Paolo, Dalla Costa Cloè, Redaelli Elena, Fabbri Alessandra, Malesci Alberto, Corrao Salvatore, Bordandini Lorella, Cereda Emanuele
Clinical Nutrition and Dietetics Unit, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy.
Clinical Nutrition and Dietetics Unit, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy.
Clin Nutr. 2022 Dec;41(12):2980-2987. doi: 10.1016/j.clnu.2021.06.020. Epub 2021 Jun 25.
BACKGROUND & AIMS: To investigate the association between the parameters used in nutritional screening assessment (body mass index [BMI], unintentional weight loss [WL] and reduced food intake) and clinical outcomes in non-critically ill, hospitalized coronavirus disease 2019 (COVID-19) patients.
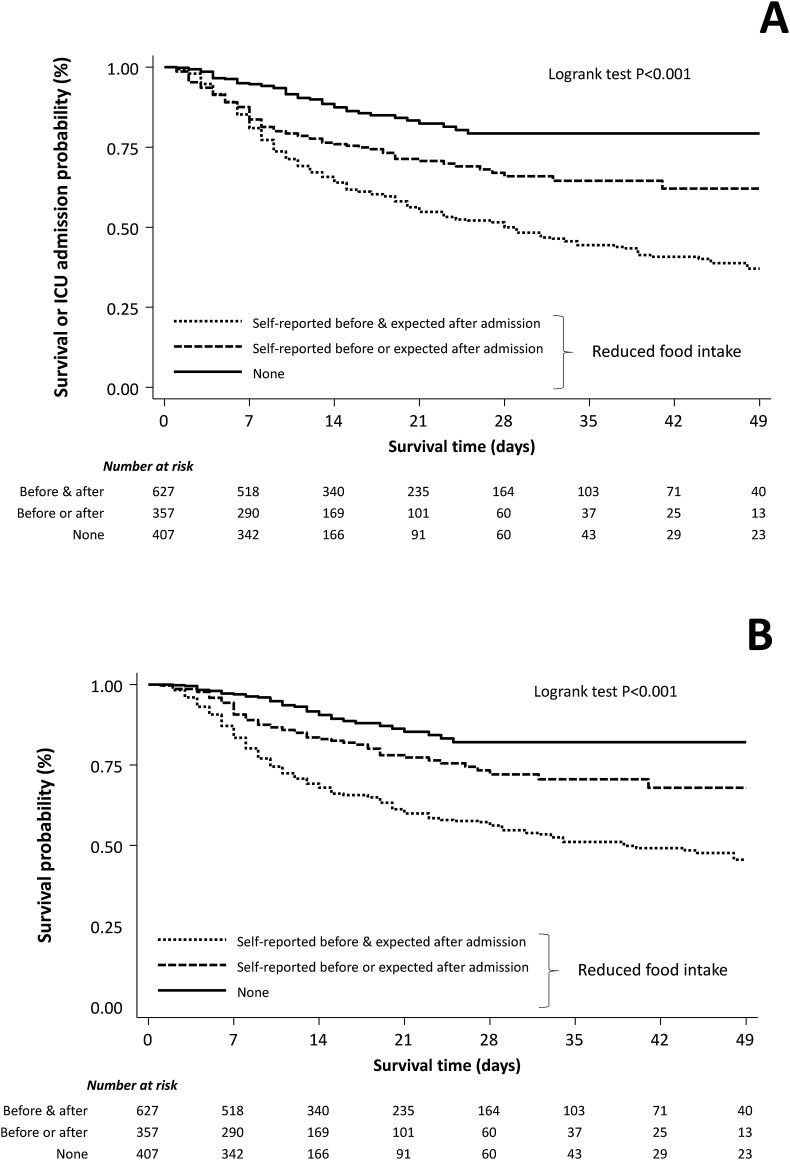
This was a prospective multicenter real-life study carried out during the first pandemic wave in 11 Italian Hospitals. In total, 1391 patients were included. The primary end-point was a composite of in-hospital mortality or admission to ICU, whichever came first. The key secondary end-point was in-hospital mortality.
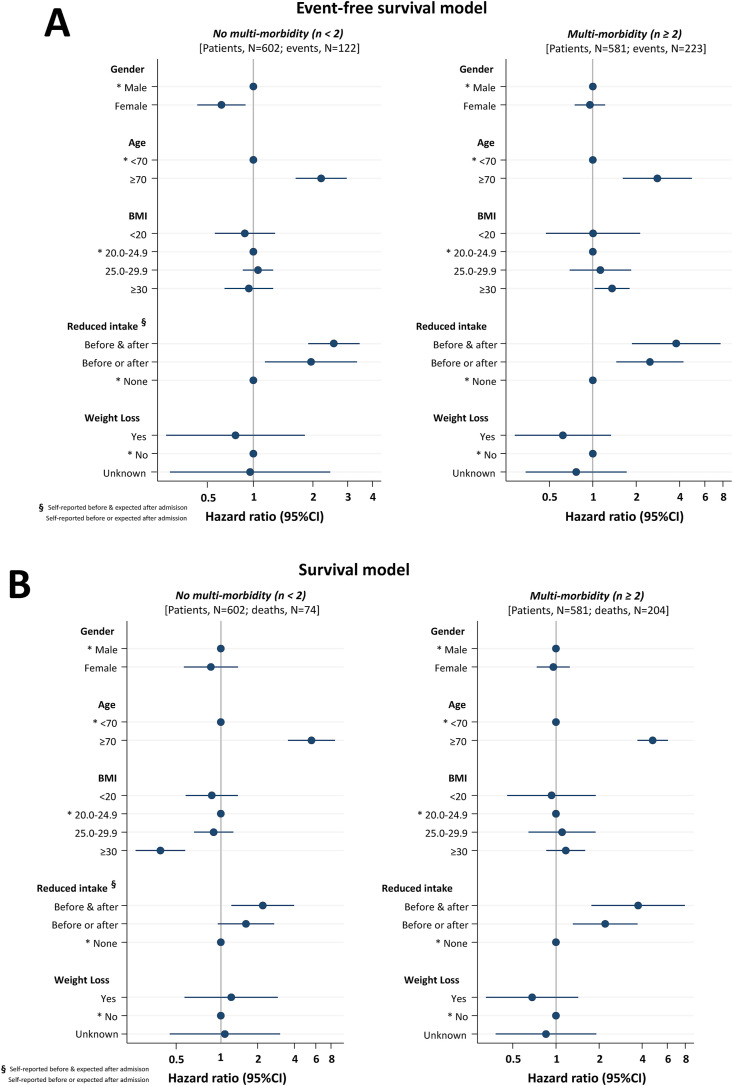
Multivariable models were based on 1183 patients with complete data. Reduced self-reported food intake before hospitalization and/or expected by physicians in the next days since admission was found to have a negative prognostic impact for both the primary and secondary end-point (P < .001 for both). No association with BMI and WL was observed. Other predictors of outcomes were age and presence of multiple comorbidities. A significant interaction between obesity and multi-morbidity (≥2) was detected. Obesity was found to be a risk factor for composite end-point (HR = 1.36 [95%CI, 1.03-1.80]; P = .031) and a protective factor against in-hospital mortality (HR = 0.32 [95%CI, 0.20-0.51]; P < .001) in patients with and without multiple comorbidities, respectively. Secondary analysis (patients, N = 829), further adjusted for high C-reactive protein (>21 mg/dL) and LDH (>430 mU/mL) levels yielded consistent findings.
Reduced self-reported food intake before hospitalization and/or expected by physicians in the next days since admission was associated with negative clinical outcomes in non-critically ill, hospitalized COVID-19 patients. This simple and easily obtainable parameter may be useful to identify patients at highest risk of poor prognosis, who may benefit from prompt nutritional support. The presence of comorbidities could be the key factor, which may determine the protective or harmful role of a high body mass index in COVID-19.
研究营养筛查评估中使用的参数(体重指数[BMI]、非故意体重减轻[WL]和食物摄入量减少)与非危重症住院的2019冠状病毒病(COVID-19)患者临床结局之间的关联。
这是一项在意大利11家医院第一波疫情期间开展的前瞻性多中心真实世界研究。共纳入1391例患者。主要终点是院内死亡或入住重症监护病房(ICU),以先发生者为准。关键次要终点是院内死亡。
多变量模型基于1183例有完整数据的患者。研究发现,入院前自我报告的食物摄入量减少和/或医生预计入院后几天内食物摄入量减少对主要和次要终点均有负面预后影响(两者P均<0.001)。未观察到与BMI和WL有关联。其他结局预测因素为年龄和多种合并症的存在。检测到肥胖与多种合并症(≥2种)之间存在显著交互作用。在有和没有多种合并症的患者中,肥胖分别被发现是复合终点的危险因素(HR = 1.36 [95%CI,1.03 - 1.80];P = 0.031)和院内死亡的保护因素(HR = 0.32 [95%CI,0.20 - 0.51];P < 0.001)。二次分析(患者,N = 829)进一步调整高C反应蛋白(>21 mg/dL)和乳酸脱氢酶(>430 mU/mL)水平后得出一致结果。
入院前自我报告的食物摄入量减少和/或医生预计入院后几天内食物摄入量减少与非危重症住院COVID-19患者的不良临床结局相关。这个简单且易于获取的参数可能有助于识别预后不良风险最高的患者,这些患者可能从及时的营养支持中获益。合并症的存在可能是关键因素,它可能决定高体重指数在COVID-19中的保护或有害作用。