Vendittoli Pascal-André, Martinov Sagi, Blakeney William G
Department of Surgery, CIUSSS-de-L'Est-de-L'Ile-de-Montréal, Hôpital Maisonneuve Rosemont, Montréal, QC, Canada.
Department of Surgery, Université de Montréal, Montréal, QC, Canada.
Front Surg. 2021 Jul 20;8:697020. doi: 10.3389/fsurg.2021.697020. eCollection 2021.
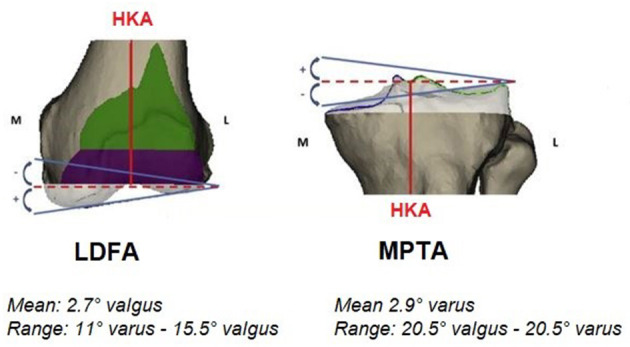
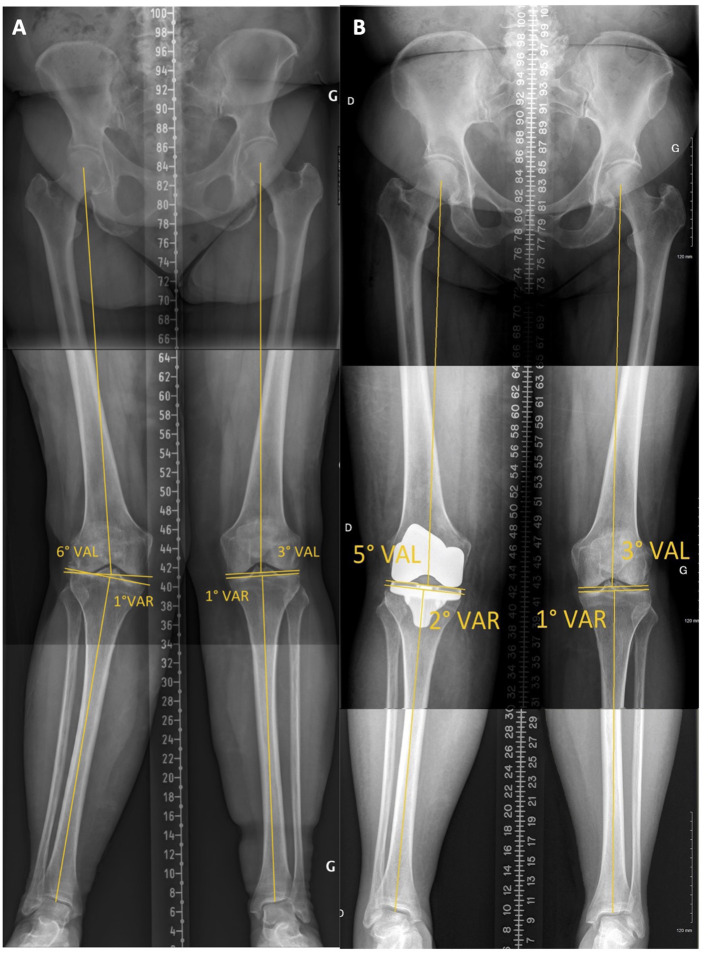
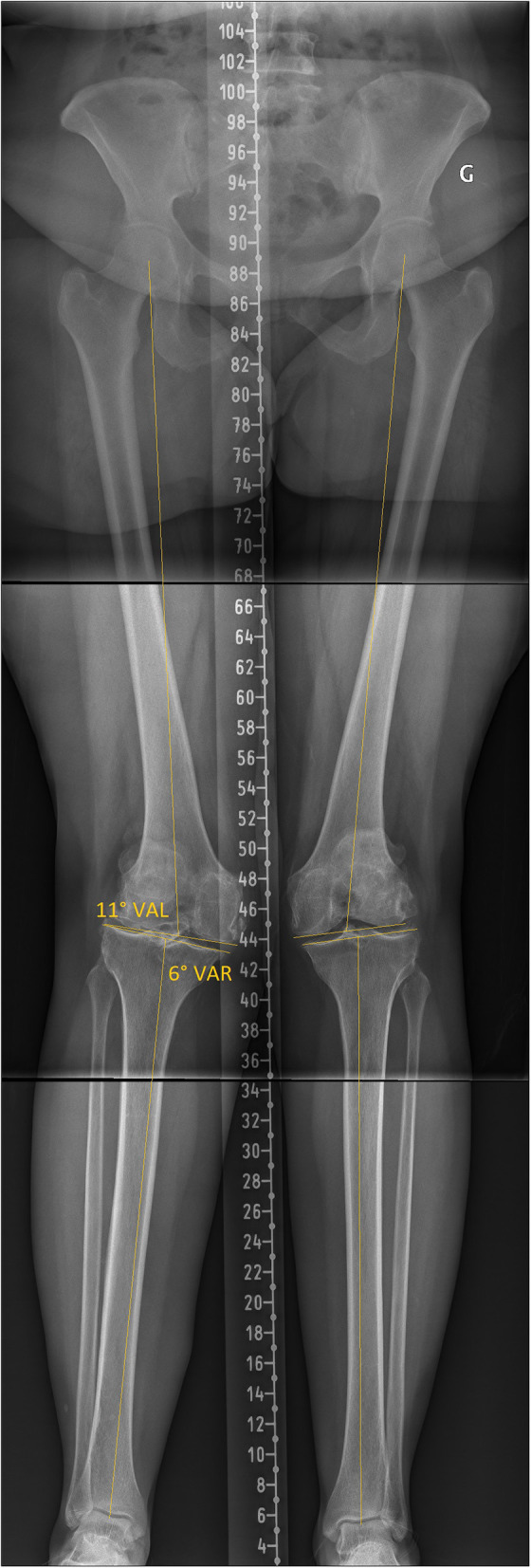
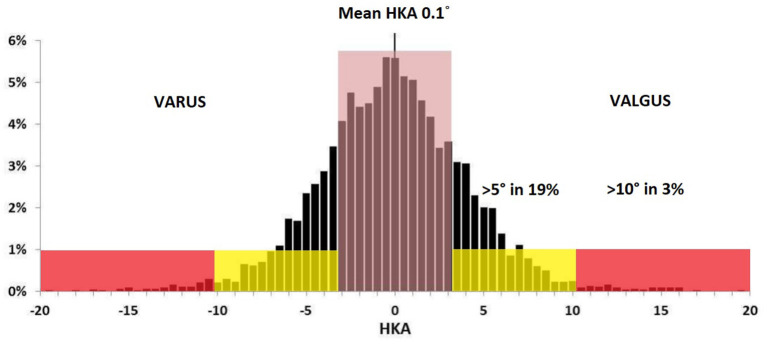
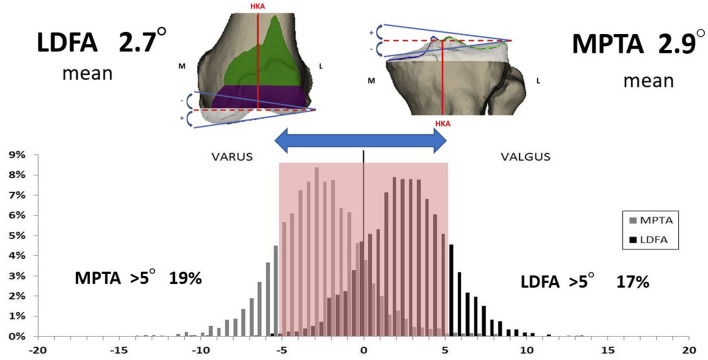
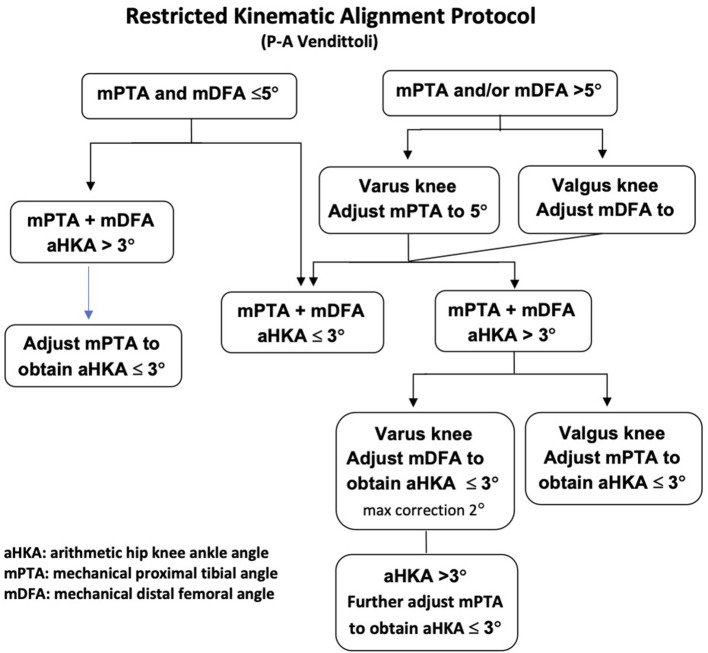
After a better understanding of normal knee anatomy and physiology, the Kinematic Alignment (KA) technique was introduced to improve clinical outcomes of total knee arthroplasty (TKA). The goal of the KA technique is to restore the pre-arthritic constitutional lower limb alignment of the patient. There is, however, a large range of normal knee anatomy. Unusual anatomies may be biomechanically inferior and affect TKA biomechanics and wear patterns. In 2011, the leading author proposed the restricted kinematic alignment (rKA) protocol, setting boundaries to KA for patients with an outlier or atypical knee anatomy. rKA aims to reproduce the constitutional knee anatomy of the patient within a safe range. Its fundamentals are based on sound comprehension of lower limb anatomy variation. There are five principles describing rKA: (1) Combined lower limb coronal orientation should be ± 3° of neutral; (2) Joint line orientation coronal alignment should be within ± 5° of neutral; (3) Natural knee's soft tissues tension/ laxities should be preserved/restored; (4) Femoral anatomy preservation is prioritized; (5) The unloaded/most intact knee compartment should be resurfaced and used as the pivot point when anatomical adjustment is required. An algorithm was developed to facilitate the decision-making. Since ~50% of patients will require anatomic modification to fit within rKA boundaries, rKA is ideally performed with patient-specific instrumentation (PSI), intra-operative computer navigation or robotic assistance. rKA surgical technique is presented in a stepwise manner, following the five principles in the algorithm. rKA produced excellent mid-term clinical results in cemented or cementless TKA. Gait analysis showed that rKA TKA patients had gait patterns that were very close to a non-operated control group, and these kinematics differences translated into significantly better postoperative patient-reported scores than mechanical alignment (MA) TKA cases. Aiming to improve the results of MA TKA, rKA protocol offers a satisfactory compromise that recreates patients' anatomy in most cases, omitting the need for extensive corrections and soft tissue releases that are often required with MA. Moreover, it precludes the reproduction of extreme anatomies seen with KA.
在对正常膝关节解剖结构和生理功能有了更深入的了解之后,运动学对线(KA)技术被引入以改善全膝关节置换术(TKA)的临床效果。KA技术的目标是恢复患者关节炎前的下肢固有对线。然而,正常膝关节解剖结构存在很大差异。异常的解剖结构可能在生物力学上较差,并影响TKA的生物力学和磨损模式。2011年,第一作者提出了受限运动学对线(rKA)方案,为膝关节解剖结构异常或不典型的患者设定了KA的界限。rKA旨在在安全范围内重现患者的固有膝关节解剖结构。其基本原理基于对下肢解剖结构变异的充分理解。有五条原则描述rKA:(1)下肢冠状面组合方向应在中立位±3°以内;(2)关节线方向冠状面对线应在中立位±5°以内;(3)应保留/恢复自然膝关节的软组织张力/松弛度;(4)优先保留股骨解剖结构;(5)当需要进行解剖学调整时,应处理无负荷/最完整的膝关节间室并将其用作枢轴点。开发了一种算法以促进决策制定。由于约50%的患者需要进行解剖学修改以符合rKA界限,rKA理想情况下应使用患者特异性器械(PSI)、术中计算机导航或机器人辅助进行。rKA手术技术按照算法中的五条原则逐步呈现。rKA在骨水泥型或非骨水泥型TKA中产生了优异的中期临床效果。步态分析表明,rKA TKA患者的步态模式与未手术的对照组非常接近,并且这些运动学差异转化为术后患者报告的评分明显优于机械对线(MA)TKA病例。旨在改善MA TKA的结果,rKA方案提供了一个令人满意的折衷方案,在大多数情况下重现患者的解剖结构,无需MA通常所需的广泛矫正和软组织松解。此外,它避免了KA中出现的极端解剖结构的重现。