From the Department of Neurosciences (L.P., S.H., C.T., C.G.), S. Camillo-Forlanini Hospital; Department of Human Neurosciences (S.R., C.P.), Sapienza University; and Neuroimmunology Unit (S.R.), Santa Lucia Foundation, Rome, Italy.
Neurol Neuroimmunol Neuroinflamm. 2021 Aug 9;8(6). doi: 10.1212/NXI.0000000000001059. Print 2021 Nov.
To estimate the proportions of patients with relapsing-remitting multiple sclerosis who despite achieving the no evidence of disease activity-3 (NEDA-3) status in the first 2 treatment years experienced relapse-associated worsening (RAW) or progression independent from relapse activity (PIRA) in the following years.
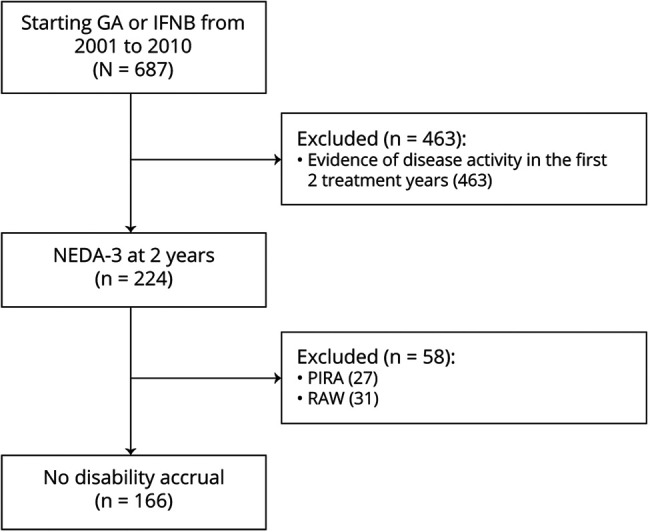
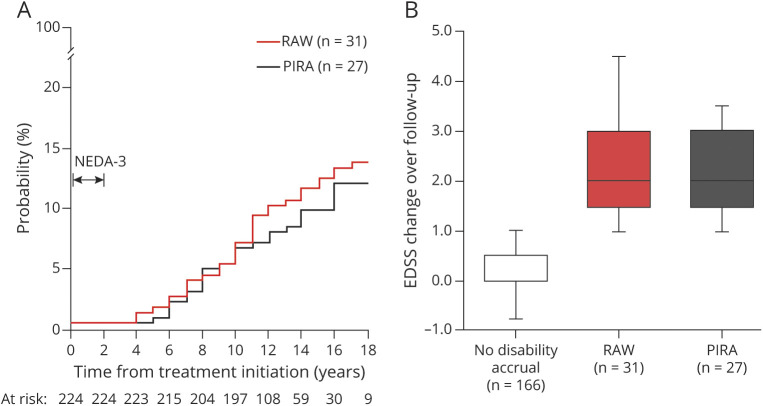
We selected patients with NEDA-3-defined as no relapse, no disability worsening, and no MRI activity-in the first 2 years of either glatiramer acetate or interferon beta as initial treatment. We estimated the long-term probability of subsequent RAW and PIRA (considered as 2 contrasting outcomes) by cumulative incidence functions. Competing risk regressions were used to identify the baseline (i.e., at treatment start) predictors of RAW and PIRA.
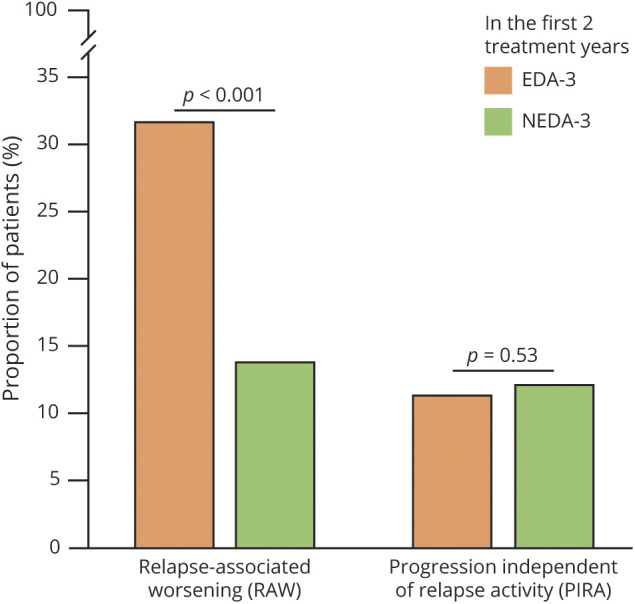
Of 687 patients, 224 (32.6%) had NEDA-3 in the first 2 treatment years. After a median follow-up time of 12 years from treatment start, 58 patients (26%) experienced disability accrual: 31 (14%) had RAW and 27 (12%) had PIRA. RAW was predicted by the presence of >9 T2 lesions (subdistribution hazard ratio [SHR] = 3.92, = 0.012) and contrast-enhancing lesions (SHR = 2.38, = 0.047) on baseline MRI scan and either temporary or permanent discontinuation of the initial treatment (SHR = 1.11, = 0.015). PIRA was predicted by advancing age (SHR = 1.05, = 0.036 for each year increase) and presence of ≥1 spinal cord lesion on baseline MRI scan (SHR = 4.08, = 0.016).
The adoption of NEDA-3 criteria led to prognostic misclassification in 1 of 4 patients. Different risk factors were associated with RAW and PIRA, suggesting alternative mechanisms for disability accrual.
This study provides Class II evidence that in patients with RRMS who attained NEDA-3 status, subsequent RAW was associated with baseline MRI activity and discontinuation of treatment and PIRA was associated with age and the presence of baseline spinal cord lesions.
评估在最初 2 年的治疗中达到无疾病活动-3(NEDA-3)状态的复发性缓解型多发性硬化症(RRMS)患者,在随后的年份中是否出现与复发相关的恶化(RAW)或与复发无关的进展(PIRA)。
我们选择了在最初 2 年内使用醋酸格拉替雷或干扰素β作为初始治疗的患者,这些患者符合 NEDA-3 定义,即无复发、无残疾恶化和无 MRI 活动。我们通过累积发病率函数估计随后发生 RAW 和 PIRA(视为 2 种对比结局)的长期概率。使用竞争风险回归来确定 RAW 和 PIRA 的基线(即治疗开始时)预测因素。
在 687 名患者中,有 224 名(32.6%)在最初 2 年的治疗中达到了 NEDA-3。从治疗开始后中位随访 12 年,有 58 名患者(26%)出现了残疾进展:31 名(14%)发生了 RAW,27 名(12%)发生了 PIRA。RAW 由基线 MRI 扫描上存在>9 个 T2 病变(亚分布危险比 [SHR] = 3.92, = 0.012)和对比增强病变(SHR = 2.38, = 0.047)、初始治疗的暂时或永久性停药(SHR = 1.11, = 0.015)预测。PIRA 由年龄增加(每增加 1 岁,SHR = 1.05, = 0.036)和基线 MRI 扫描上存在≥1 个脊髓病变(SHR = 4.08, = 0.016)预测。
采用 NEDA-3 标准导致 1/4 的患者出现预后误分类。RAW 和 PIRA 与不同的危险因素相关,提示残疾进展的机制不同。
本研究提供了 II 级证据,表明在达到 NEDA-3 状态的 RRMS 患者中,随后的 RAW 与基线 MRI 活动和治疗停药有关,而 PIRA 与年龄和基线脊髓病变有关。