Department of Diagnostic and Interventional Radiology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Kerpener Str. 62, 50937, Cologne, Germany.
Department of Radiology, Harvard Medical School, Massachusetts General Hospital, 55 Fruit St, White 270, Boston, MA, 02114, USA.
Sci Rep. 2021 Aug 12;11(1):16437. doi: 10.1038/s41598-021-95962-z.
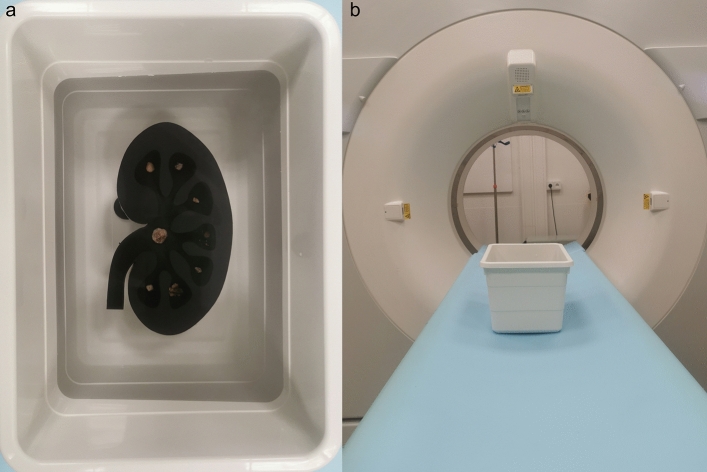
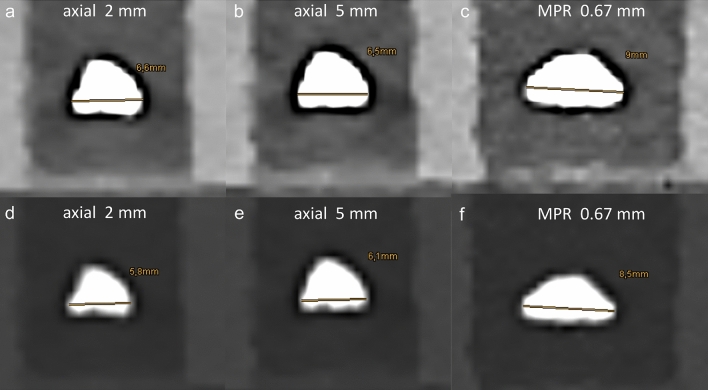
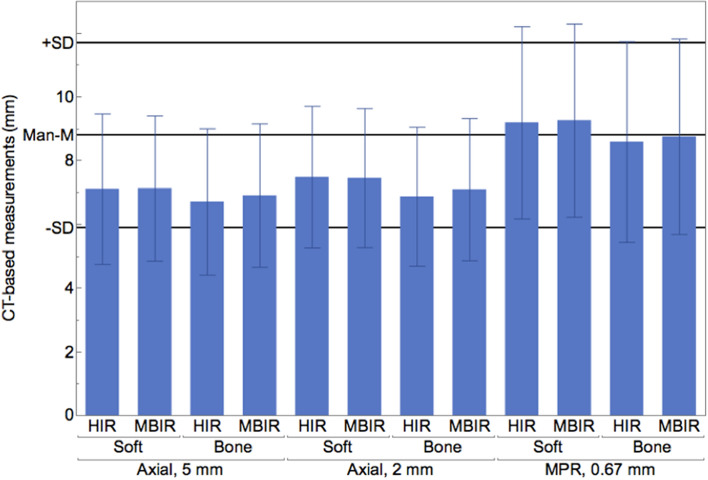
Computed tomography in suspected urolithiasis provides information about the presence, location and size of stones. Particularly stone size is a key parameter in treatment decision; however, data on impact of reformatation and measurement strategies is sparse. This study aimed to investigate the influence of different image reformatations, slice thicknesses and window settings on stone size measurements. Reference stone sizes of 47 kidney stones representative for clinically encountered compositions were measured manually using a digital caliper (Man-M). Afterwards stones were placed in a 3D-printed, semi-anthropomorphic phantom, and scanned using a low dose protocol (CTDI 2 mGy). Images were reconstructed using hybrid-iterative and model-based iterative reconstruction algorithms (HIR, MBIR) with different slice thicknesses. Two independent readers measured largest stone diameter on axial (2 mm and 5 mm) and multiplanar reformatations (based upon 0.67 mm reconstructions) using different window settings (soft-tissue and bone). Statistics were conducted using ANOVA ± correction for multiple comparisons. Overall stone size in CT was underestimated compared to Man-M (8.8 ± 2.9 vs. 7.7 ± 2.7 mm, p < 0.05), yet closely correlated (r = 0.70). Reconstruction algorithm and slice thickness did not significantly impact measurements (p > 0.05), while image reformatations and window settings did (p < 0.05). CT measurements using multiplanar reformatation with a bone window setting showed closest agreement with Man-M (8.7 ± 3.1 vs. 8.8 ± 2.9 mm, p < 0.05, r = 0.83). Manual CT-based stone size measurements are most accurate using multiplanar image reformatation with a bone window setting, while measurements on axial planes with different slice thicknesses underestimate true stone size. Therefore, this procedure is recommended when impacting treatment decision.
在疑似尿路结石的情况下,计算机断层扫描可提供有关结石存在、位置和大小的信息。特别是结石大小是治疗决策的关键参数;然而,关于图像重建成像和测量策略的影响的数据却很少。本研究旨在调查不同的图像重建成像、层厚和窗宽设置对结石大小测量的影响。使用数字卡尺(Man-M)手动测量 47 颗具有代表性的临床结石来获得参考结石大小。然后将结石放置在 3D 打印的半拟人化体模中,使用低剂量方案(CTDI 2 mGy)进行扫描。使用混合迭代和基于模型的迭代重建算法(HIR、MBIR)对图像进行不同层厚的重建。两名独立的读者使用不同的窗宽(软组织和骨)在轴位(2mm 和 5mm)和多平面重建成像(基于 0.67mm 重建)上测量最大结石直径。使用方差分析(ANOVA)进行统计学分析,并对多重比较进行校正。与 Man-M 相比,CT 中的总体结石大小被低估(8.8±2.9 vs. 7.7±2.7mm,p<0.05),但相关性很好(r=0.70)。重建算法和层厚对测量结果没有显著影响(p>0.05),而图像重建成像和窗宽设置则有影响(p<0.05)。使用多平面重建成像和骨窗设置的 CT 测量与 Man-M 最接近(8.7±3.1 vs. 8.8±2.9mm,p<0.05,r=0.83)。使用多平面图像重建成像和骨窗设置进行基于 CT 的结石大小手动测量最准确,而使用不同层厚的轴位图像测量则会低估真实的结石大小。因此,在影响治疗决策时,建议采用这种方法。