Kim Whoan Jeang, Ma Sang Beom, Shin Hyun Min, Song Dae Geon, Lee Jae Won, Chang Shan Haw, Park Kun Young, Choy Won Sik, Oh Tae Ho
Department of Orthopedic Surgery, Eulji University School of Medicine, Daejeon, Korea.
Asian Spine J. 2022 Apr;16(2):231-240. doi: 10.31616/asj.2021.0062. Epub 2021 Aug 20.
A retrospective case control study.
This study aimed to assess the clinical significance of sagittal balance for predicting and managing the recollapse of cemented vertebra following percutaneous vertebroplasty (PVP) in patients with thoracolumbar osteoporotic vertebral fracture (OVF).
Recently, the recollapse of cemented vertebra following PVP for OVF has been reported. Although the risk factors for recollapse have been determined, the association between sagittal spinopelvic parameters and sagittal imbalance with recollapse has not been established.
Ambulatory patients who underwent single-level PVP for thoracolumbar OVF with a follow-up of at least 24 months were retrospectively reviewed. The patients were divided into two groups depending on the presence of symptomatic recollapse at the cemented vertebra: (1) recollapsed (RC) group and (2) noncollapsed (NC) group. The patient characteristics and radiographic measurements associated with sagittal imbalance were analyzed at each follow-up visit.
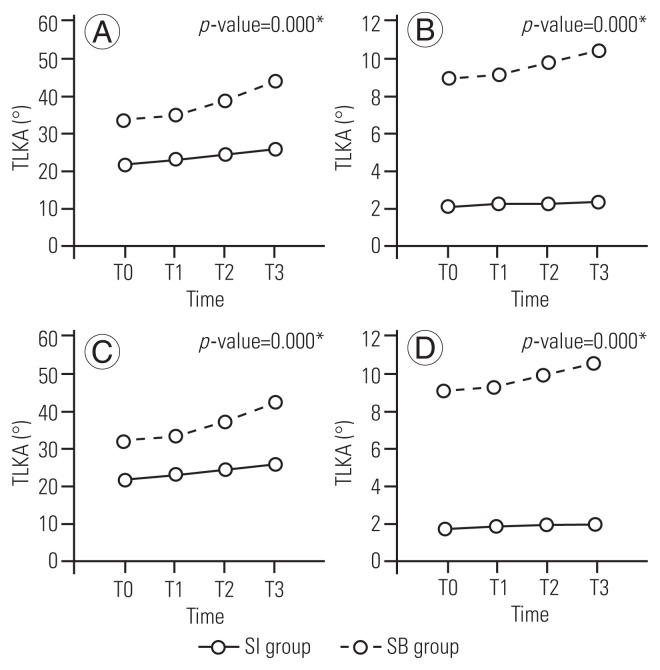
Overall, 134 patients (RC group, n=28; NC group, n=106) were enrolled. The mean fracture-free interval was 3.2 months (range, 1.2-25.1 months). The multivariate binary logistic regression analysis identified low bone mineral density (p =0.047), degree of dynamic mobility within the vertebra (p =0.025), and sagittal imbalance as significant risk factors for recollapse (p =0.013; odds ratio, 5.405). The progression of sagittal imbalance and thoracolumbar kyphosis (T10-L2) was more significant in the RC and sagittal imbalance groups than in the NC group (both p =0.000).
Sagittal imbalance, lower bone mineral density, and dynamic mobility within the vertebra are associated with the recollapse of cemented vertebrae following PVP. Sagittal imbalance, rather than local kyphosis or thoracolumbar kyphosis, is particularly significant in that it results in more progressive collapse and sagittal deformity and is accompanied by substantial back pain and neurological deficits. Therefore, a stricter and more active management, including anti-osteoporosis medication, is required for the treatment of OVF with sagittal imbalance of the spine.
一项回顾性病例对照研究。
本研究旨在评估矢状面平衡对于预测和处理胸腰椎骨质疏松性椎体骨折(OVF)患者经皮椎体成形术(PVP)后骨水泥强化椎体再塌陷的临床意义。
最近,已有关于OVF患者PVP后骨水泥强化椎体再塌陷的报道。尽管已确定再塌陷的危险因素,但矢状面脊柱骨盆参数和矢状面失衡与再塌陷之间的关联尚未明确。
对接受单节段胸腰椎OVF的PVP且随访至少24个月的门诊患者进行回顾性分析。根据骨水泥强化椎体是否出现有症状的再塌陷,将患者分为两组:(1)再塌陷(RC)组和(2)未塌陷(NC)组。在每次随访时分析与矢状面失衡相关的患者特征和影像学测量结果。
共纳入134例患者(RC组,n = 28;NC组,n = 106)。平均无骨折间隔时间为3.2个月(范围1.2 - 25.1个月)。多因素二元逻辑回归分析确定低骨密度(p = 0.047)、椎体内动态活动度(p = 0.025)和矢状面失衡是再塌陷的重要危险因素(p = 0.013;比值比,5.405)。RC组和矢状面失衡组的矢状面失衡和胸腰椎后凸(T10 - L2)进展比NC组更显著(均p = 0.000)。
矢状面失衡、较低的骨密度和椎体内动态活动度与PVP后骨水泥强化椎体再塌陷相关。矢状面失衡,而非局部后凸或胸腰椎后凸,尤为重要,因为它会导致更渐进性的塌陷和矢状面畸形,并伴有严重的背痛和神经功能缺损。因此,对于存在脊柱矢状面失衡的OVF患者,需要更严格、更积极的治疗,包括抗骨质疏松药物治疗。