Department of Orthopaedic Surgery and Traumatology, Lillebaelt Hospital, University Hospital of Southern Denmark, Sygehusvej 24, 6000, Kolding, Denmark.
Department of Orthopaedic Surgery, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
Syst Rev. 2021 Aug 18;10(1):234. doi: 10.1186/s13643-021-01785-4.
Several comorbidity indices have been created to estimate and adjust for the burden of comorbidity. The objective of this systematic review was to evaluate and compare the ability of different comorbidity indices to predict mortality in an orthopedic setting.
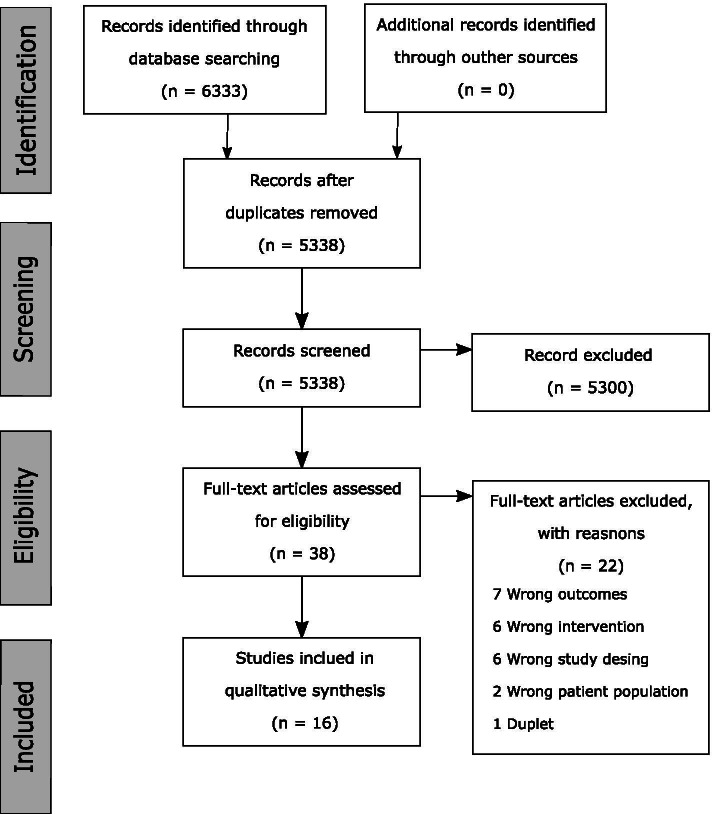
A systematic search was conducted in Embase, MEDLINE, and Cochrane Library. The search were constructed around two primary focal points: a comorbidity index and orthopedics. The last search were performed on 13 June 2019. Eligibility criteria were participants with orthopedic conditions or who underwent an orthopedic procedure, a comparison between comorbidity indices that used administrative data, and reported mortality as outcome. Two independent reviewers screened the studies using Covidence. The area under the curve (AUC) was chosen as the primary effect estimate.
Of the 5338 studies identified, 16 met the eligibility criteria. The predictive ability of the different comorbidity indices ranged from poor (AUC < 0.70) to excellent (AUC ≥ 0.90). The majority of the included studies compared the Elixhauser Comorbidity Index (ECI) and the Charlson Comorbidity Index (CCI). In-hospital mortality was reported in eight studies reporting AUC values ranging from 0.70 to 0.92 for ECI and 0.68 to 0.89 for CCI. AUC values were generally lower for all other time points ranging from 0.67 to 0.78. For 1-year mortality the overall effect size ranging from 0.67 to 0.77 for ECI and 0.69 to 0.77 for CCI.
The results of this review indicate that the ECI and CCI can equally be used to adjust for comorbidities when analyzing mortality in an orthopedic setting.
The protocol for this systematic review was registered on PROSPERO, the International Prospective Register of Systematic Reviews on 13 June 2019 and can be accessed through record ID 133,871.
已经创建了几种合并症指数来估计和调整合并症的负担。本系统评价的目的是评估和比较不同合并症指数预测骨科环境下死亡率的能力。
在 Embase、MEDLINE 和 Cochrane 图书馆中进行了系统搜索。搜索围绕两个主要焦点构建:合并症指数和骨科。最后一次搜索于 2019 年 6 月 13 日进行。纳入标准为患有骨科疾病或接受骨科手术的患者、使用行政数据的合并症指数比较、并报告死亡率为结局。两名独立评审员使用 Covidence 筛选研究。曲线下面积(AUC)被选为主要效应估计。
在确定的 5338 项研究中,有 16 项符合纳入标准。不同合并症指数的预测能力从较差(AUC<0.70)到较好(AUC≥0.90)不等。大多数纳入的研究比较了 Elixhauser 合并症指数(ECI)和 Charlson 合并症指数(CCI)。有 8 项研究报告了 AUC 值,范围为 0.70 至 0.92 的 ECI 和 0.68 至 0.89 的 CCI,报告了住院死亡率。对于所有其他时间点,AUC 值通常较低,范围为 0.67 至 0.78。对于 1 年死亡率,总体效应大小为 0.67 至 0.77 的 ECI 和 0.69 至 0.77 的 CCI。
本研究结果表明,在分析骨科环境下的死亡率时,ECI 和 CCI 可以同样用于调整合并症。
本系统评价的方案于 2019 年 6 月 13 日在 PROSPERO,国际系统评价前瞻性注册库中注册,可以通过记录 ID 133871 访问。