Department of Cardiovascular Medicine The University of Kansas Health SystemUniversity of Kansas School of Medicine Kansas City KS.
The Cardiovascular Center Tufts Medical Center Tufts University School of Medicine Boston MA.
J Am Heart Assoc. 2021 Sep 7;10(17):e019843. doi: 10.1161/JAHA.120.019843. Epub 2021 Aug 21.
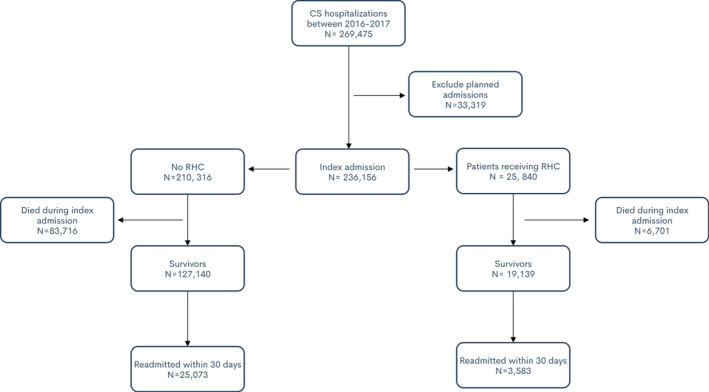
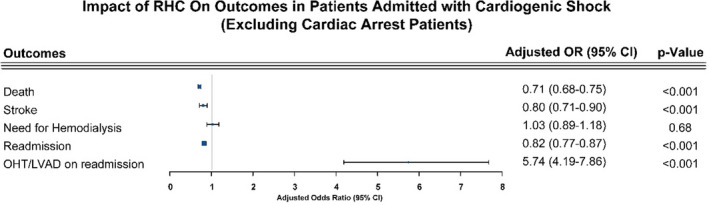
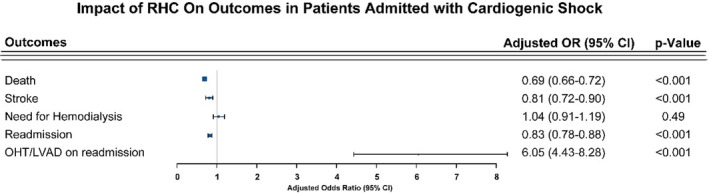
Background The usefulness of right heart catherization (RHC) has long been debated, and thus, we aimed to study the real-world impact of the use of RHC in cardiogenic shock. Methods and Results In the Nationwide Readmissions Database using (), we identified 236 156 patient hospitalizations with cardiogenic shock between 2016 and 2017. We sought to evaluate the impact of RHC during index hospitalization on management strategies, complications, and outcomes as well as on 30-day readmission rate. A total 25 840 patients (9.6%) received RHC on index admission. The RHC group had significantly more comorbidities compared with the non-RHC group. During the index admission, the RHC group had lower death (25.8% versus 39.5%, <0.001) and stroke rates (3.1% versus 3.4%, <0.001). Thirty-day readmission rates (18.7% versus 19.7%, =0.04) and death on readmission (7.9% versus 9.3%, =0.03) were also lower in the RHC group. After adjustment, RHC was associated with lower index admission mortality (odds ratio, 0.69; 95% CI, 0.66-0.72), lower stroke rate (odds ratio, 0.81; 95% CI, 0.72-0.90), lower 30-day readmission (odds ratio, 0.83; 95% CI, 0.78-0.88), and higher left ventricular assist device implantations/orthotopic heart transplants (odds ratio, 6.05; 95% CI, 4.43-8.28) during rehospitalization. Results were not meaningfully different after excluding patients with cardiac arrest. Conclusions RHC use in cardiogenic shock is associated with improved outcomes and increased use of downstream advanced heart failure therapies. Further blinded randomized studies are required to confirm our findings.
右心导管检查(RHC)的有效性一直存在争议,因此,我们旨在研究在心源性休克患者中使用 RHC 的实际影响。
我们使用()在全国再入院数据库中,确定了 2016 年至 2017 年间 236156 例心源性休克患者的住院治疗。我们试图评估指数住院期间 RHC 对管理策略、并发症和结局以及 30 天再入院率的影响。共有 25840 例患者(9.6%)在指数入院时接受 RHC。RHC 组与非 RHC 组相比,合并症明显更多。在指数住院期间,RHC 组的死亡率(25.8%对 39.5%,<0.001)和卒中率(3.1%对 3.4%,<0.001)明显更低。RHC 组 30 天再入院率(18.7%对 19.7%,=0.04)和再入院死亡率(7.9%对 9.3%,=0.03)也较低。调整后,RHC 与指数入院死亡率降低相关(比值比,0.69;95%置信区间,0.66-0.72)、卒中率降低(比值比,0.81;95%置信区间,0.72-0.90)、30 天再入院率降低(比值比,0.83;95%置信区间,0.78-0.88)和心脏辅助装置植入/原位心脏移植增加(比值比,6.05;95%置信区间,4.43-8.28)。排除心脏骤停患者后,结果差异无统计学意义。
心源性休克患者使用 RHC 可改善结局,并增加晚期心力衰竭治疗的应用。需要进一步进行盲法随机研究来证实我们的发现。