Rao Fudong, Wang Zongjie, Chen Xijuan, Liu Linwei, Qian Bin, Guo Yanhua
Department of Anesthesiology, People's Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People's Republic of China.
Department of Anesthesiology, Longyan First Hospital Affiliated to Fujian Medical University, Longyan, Fujian, People's Republic of China.
J Pain Res. 2021 Aug 20;14:2563-2570. doi: 10.2147/JPR.S325627. eCollection 2021.
Ultrasound-guided thoracic paravertebral block (TPVB) has become increasingly popular for postoperative analgesia after breast surgery. We designed this prospective, randomized, double-blind, placebo-controlled trial to test the hypothesis that TPVB is superior to placebo in improving the patient quality of recovery following modified radical mastectomy.
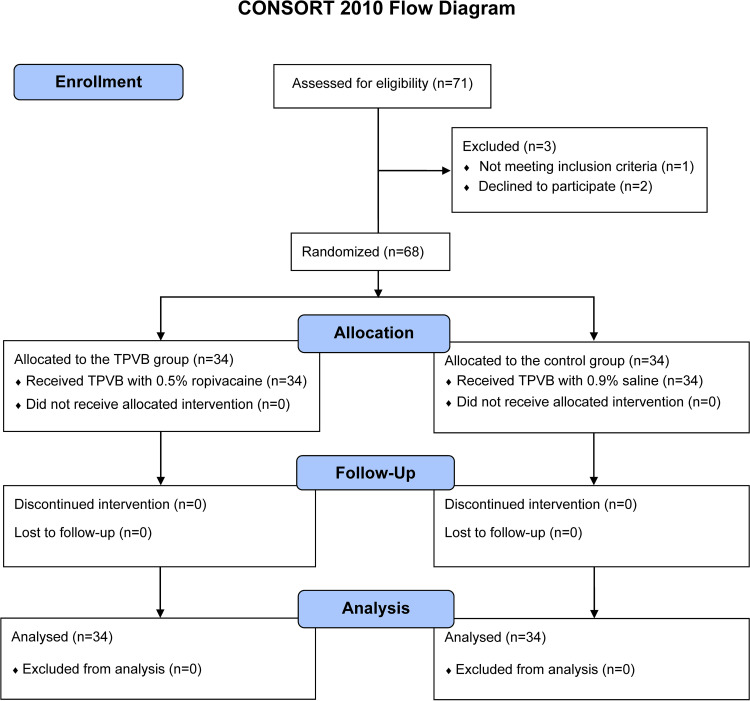
Sixty-eight female patients undergoing elective unilateral modified radical mastectomy were enrolled. Patients were randomized to receive preoperative ultrasound-guided TPVB with 0.5% ropivacaine (TPVB group, n=34) or 0.9% saline (Control group, n=34). The primary outcome was quality of recovery, measured 24 h after surgery using the 40-item Quality of recovery questionnaire (QoR-40). Secondary outcomes were the area under the curve of the visual analog scale pain scores over 24 h, postoperative 24-h morphine consumption, time to first rescue analgesia, length of post-anesthesia care unit stay, postoperative nausea and vomiting, and patient satisfaction.
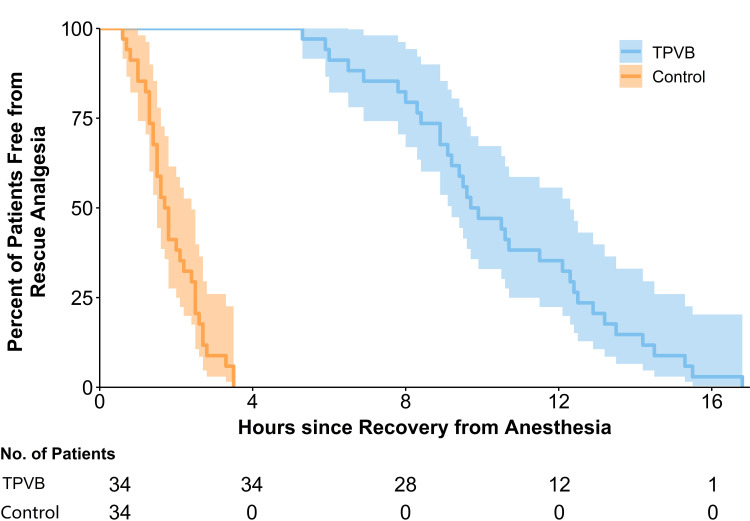
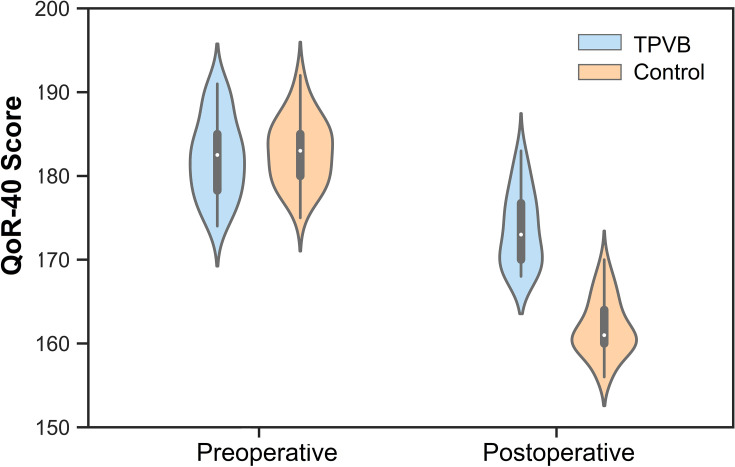
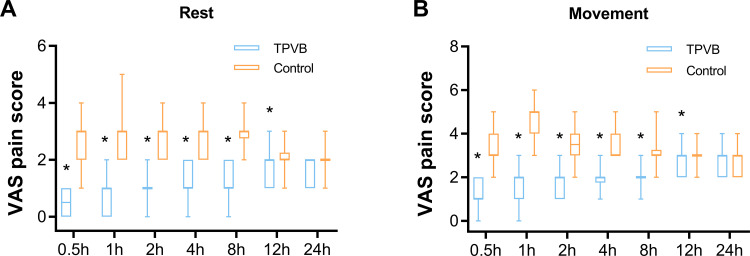
The global QoR-40 score 24 h postoperatively (median [interquartile range]) was 173 [170-177] in the TPVB group and 161 [160-164] in the control group (<0.001), respectively, with a median difference (95% confidence interval) of 11 (9-14). Compared with the control group, preoperative TPVB decreased the area under the curve of the visual analog scale pain scores over 24 h, reduced postoperative 24-h morphine consumption, prolonged the time to first rescue analgesia, shortened the length of post-anesthesia care unit stay, lessened postoperative nausea and vomiting, and improved the patient satisfaction.
A single preoperative injection of TPVB with ropivacaine enhances the quality of recovery and postoperative analgesia in patients following modified radical mastectomy.
超声引导下胸椎旁神经阻滞(TPVB)在乳腺癌手术后的术后镇痛中越来越受欢迎。我们设计了这项前瞻性、随机、双盲、安慰剂对照试验,以检验以下假设:在改良根治性乳房切除术后,TPVB在改善患者恢复质量方面优于安慰剂。
纳入68例行择期单侧改良根治性乳房切除术的女性患者。患者被随机分为两组,分别在术前接受超声引导下注射0.5%罗哌卡因的TPVB(TPVB组,n = 34)或0.9%生理盐水(对照组,n = 34)。主要结局是恢复质量,在术后24小时使用40项恢复质量问卷(QoR - 40)进行测量。次要结局包括24小时视觉模拟量表疼痛评分的曲线下面积、术后24小时吗啡消耗量、首次补救镇痛时间、麻醉后护理单元停留时间、术后恶心呕吐以及患者满意度。
术后24小时,TPVB组的全球QoR - 40评分(中位数[四分位间距])为173[170 - 177],对照组为161[160 - 164](<0.001),中位数差异(95%置信区间)为11(9 - 14)。与对照组相比,术前TPVB降低了24小时视觉模拟量表疼痛评分的曲线下面积,减少了术后24小时吗啡消耗量,延长了首次补救镇痛时间,缩短了麻醉后护理单元停留时间,减轻了术后恶心呕吐,并提高了患者满意度。
术前单次注射罗哌卡因进行TPVB可提高改良根治性乳房切除术后患者的恢复质量和术后镇痛效果。