Department of Psychology, Georgia State University, Atlanta, GA, 30302-5010, USA.
Smith+Nephew, 155 Jefferson Drive, Menlo Park, CA, 94025, USA.
J Clin Psychol Med Settings. 2022 Jun;29(2):285-294. doi: 10.1007/s10880-021-09813-0. Epub 2021 Aug 31.
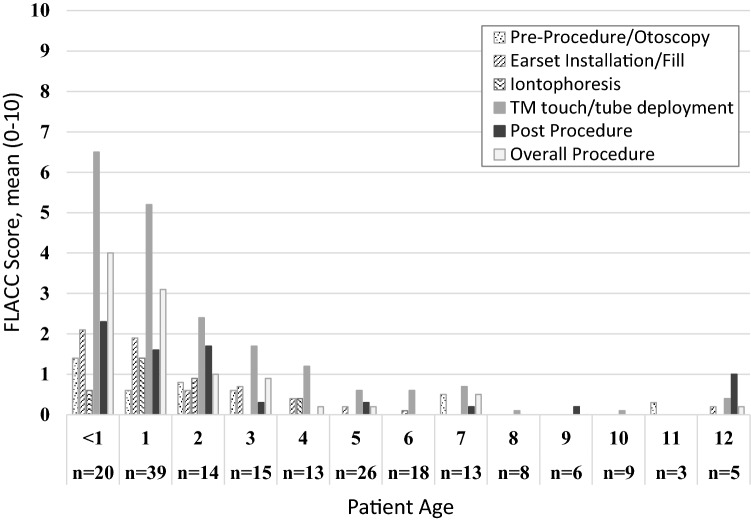
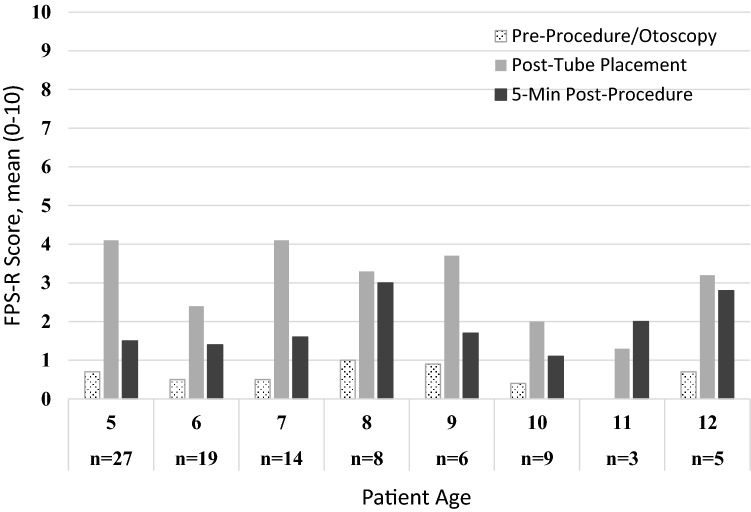
The purpose of this study was to evaluate behavioral strategies to minimize procedural distress associated with in-office tympanostomy tube placement for children without general anesthesia, sedation, or papoose-board restraints. 120 6-month- to 4-year-olds and 102 5- to 12-year-olds were treated at 16 otolaryngology practices. Mean age of children was 4.7 years old (SD = 3.18 years), with more boys (58.1%) than girls (41.9%). The cohort included 14% Hispanic or Latinx, 84.2% White, 12.6% Black, 1.8% Asian and 4.1% 'Other' race and ethnicity classifications. The in-office tube placement procedure included local anesthesia via lidocaine/epinephrine iontophoresis and tube placement using an integrated and automated myringotomy and tube delivery system. Behavioral strategies were used to minimize procedural distress. Anxiolytics, sedation, or papoose board were not used. Pain was measured via the faces pain scale-revised (FPS-R) self-reported by the children ages 5 through 12 years. Independent coders supervised by a psychologist completed the face, legs, activity, cry, consolability (FLACC) behavior observational rating scale to quantify children's distress. Mean FPS-R score for tube placement was 3.30, in the "mild' pain range, and decreased to 1.69 at 5-min post-procedure. Mean tube placement FLACC score was 4.0 (out of a maximum score of 10) for children ages 6 months to 4 years and was 0.4 for children age 5-12 years. Mean FLACC score 3-min post-tube placement was 1.3 for children ages 6 months to 4 years and was 0.2 for children age 5-12 years. FLACC scores were inversely correlated with age, with older children displaying lower distress. The iontophoresis, tube delivery system and behavioral program were associated with generally low behavioral distress. These data suggest that pediatric tympanostomy and tube placement can be achieved in the outpatient setting without anxiolytics, sedatives, or mechanical restraints.
本研究旨在评估行为策略,以最小化门诊鼓膜置管术相关的程序痛苦,适用于无需全身麻醉、镇静或约束带的儿童。16 个耳鼻喉科诊所共治疗了 120 名 6 个月至 4 岁和 102 名 5 至 12 岁的儿童。患儿平均年龄为 4.7 岁(标准差=3.18 岁),男孩(58.1%)多于女孩(41.9%)。该队列包括 14%的西班牙裔或拉丁裔,84.2%的白人,12.6%的黑人,1.8%的亚洲人和 4.1%的其他种族和民族分类。门诊置管过程包括通过利多卡因/肾上腺素离子电渗疗法进行局部麻醉,以及使用集成和自动化鼓膜切开和管输送系统进行管放置。采用行为策略来最小化程序痛苦。未使用安定、镇静剂或约束带。5 至 12 岁的儿童通过面部疼痛量表修订版(FPS-R)自我报告来测量疼痛。由心理学家监督的独立编码员完成面部、腿部、活动、哭泣、安抚性(FLACC)行为观察评分量表,以量化儿童的痛苦。管放置的平均 FPS-R 评分为 3.30,处于“轻度”疼痛范围,术后 5 分钟降至 1.69。6 个月至 4 岁儿童的平均管放置 FLACC 评分为 4.0(满分 10 分),5-12 岁儿童的评分为 0.4。管放置后 3 分钟,6 个月至 4 岁儿童的平均 FLACC 评分为 1.3,5-12 岁儿童的评分为 0.2。FLACC 评分与年龄呈负相关,年龄较大的儿童表现出较低的痛苦。离子电渗疗法、管输送系统和行为方案与一般较低的行为痛苦相关。这些数据表明,儿科鼓膜切开和置管术可以在门诊环境中完成,无需使用安定剂、镇静剂或机械约束。