Department of Epidemiology and Biostatistics, Arnold School of Public Health, University of South Carolina, Columbia, SC, USA.
Department of Psychology, University of South Carolina, Columbia, SC, USA.
J Am Med Dir Assoc. 2021 Oct;22(10):2026-2031.e1. doi: 10.1016/j.jamda.2021.08.006. Epub 2021 Aug 16.
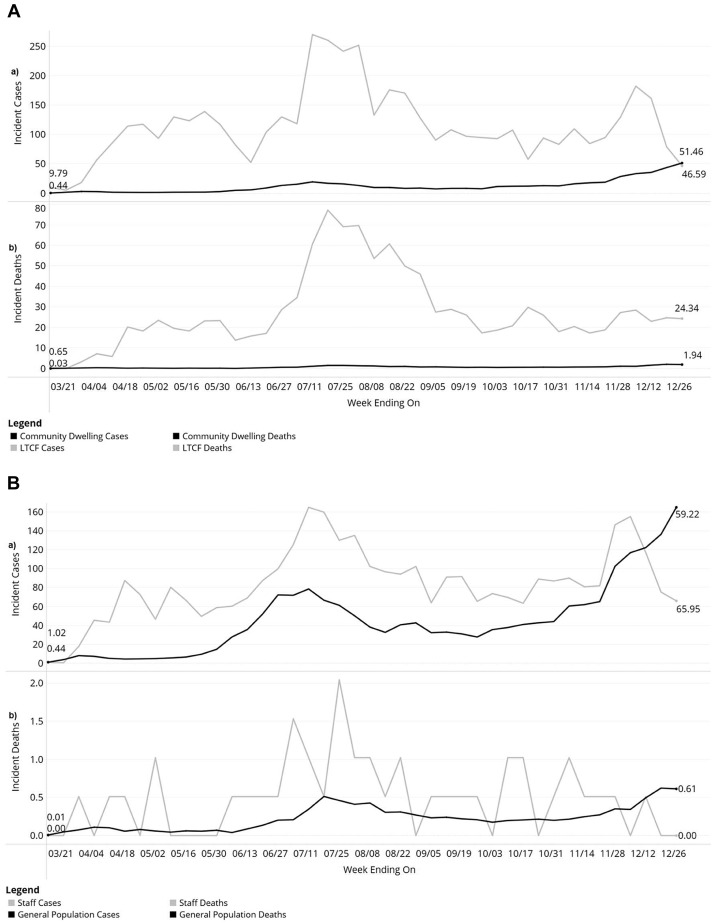
This study explored differences in COVID-19 incidence, mortality, and timing among long-term care facility (LTCF) residents and staff with those living in the community in South Carolina (SC).
Longitudinal secondary data analysis.
Adults age ≥18 in SC with confirmed COVID-19 diagnosis from 3/15/2020 and 1/2/2021 (n = 307,891).
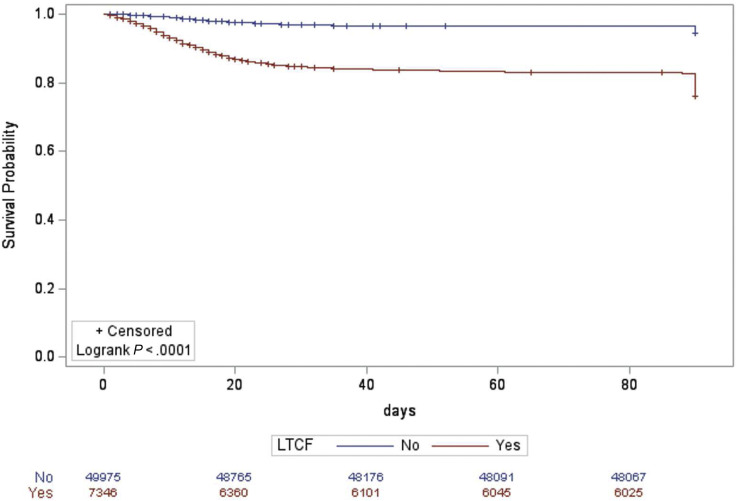
COVID-19 data came from the SC Department of Health and Environmental Control (SCDHEC). We included all COVID-19 cases, hospitalizations, and deaths among adult residents. Residence and employment in LTCF were confirmed by SCDHEC. Descriptive statistics and trends for cases, hospitalizations, and deaths were calculated. We used Cox proportional hazards to compare COVID-19 mortality in LTCF residents and staff to community dwelling older adults and adults not employed in LTCF, respectively, controlling for age, gender, race, and pre-existing chronic health conditions.
LTC residents experienced greater incidence of cases throughout the study period until the week ending on 1/2/21. LTCF residents with COVID-19 were more likely to be hospitalized compared to older adults in the community and 74% more likely to die (HR: 1.74, 95% CI: 1.59-1.90), after adjusting. LTC staff experienced greater incidence of cases compared to adults not employed in LTCF until the week ending on 12/26/2020, while experiencing similar incidence of death compared to the similar community members. After adjusting, LTC staff had 0.58 (HR = 0.58; CI: 0.39-0.88) times lower hazard of death compared to community members that did not work in a LTCF.
Narrowing of the gap between LTCF and community-wide infection and mortality rates over the study period suggests that early detection of COVID-19 in LTCFs could serve as a first indicator of disease spread in the greater community. Results also indicate that policies and regulations addressing staff testing and protection may help to slow or prevent spread within facilities.
本研究旨在探讨南卡罗来纳州(SC)长期护理机构(LTCF)居民和工作人员与社区居民的 COVID-19 发病率、死亡率和发病时间的差异。
纵向二次数据分析。
年龄≥18 岁的成年人,在 2020 年 3 月 15 日至 2021 年 1 月 2 日期间在 SC 经确诊患有 COVID-19(n=307891)。
COVID-19 数据来自南卡罗来纳州卫生与环境控制部(SCDHEC)。我们纳入了所有成年居民的 COVID-19 病例、住院和死亡病例。SCDHEC 确认了 LTCF 的居住和就业情况。计算了病例、住院和死亡的描述性统计数据和趋势。我们使用 Cox 比例风险模型分别比较了 LTCF 居民和工作人员的 COVID-19 死亡率与社区居住的老年人和未在 LTCF 工作的成年人,同时控制了年龄、性别、种族和预先存在的慢性健康状况。
在整个研究期间,LTC 居民的病例发生率一直较高,直到 2021 年 1 月 2 日结束的那一周。与社区中的老年人相比,患有 COVID-19 的 LTCF 居民更有可能住院,并且死亡的可能性高 74%(HR:1.74,95%CI:1.59-1.90),调整后。与未在 LTCF 工作的成年人相比,LTC 工作人员的病例发生率在 2020 年 12 月 26 日结束的那一周一直较高,而与类似的社区成员相比,死亡发生率相似。调整后,LTC 工作人员的死亡风险比未在 LTCF 工作的社区成员低 0.58(HR=0.58;CI:0.39-0.88)。
在研究期间,LTCF 和社区范围内的感染和死亡率之间的差距缩小表明,早期发现 LTCF 中的 COVID-19 可能成为疾病在更大社区传播的第一个指标。结果还表明,解决员工检测和保护的政策和法规可能有助于减缓或防止设施内的传播。