Sanfilippo Filippo, La Via Luigi, Lanzafame Bruno, Dezio Veronica, Busalacchi Diana, Messina Antonio, Ristagno Giuseppe, Pelosi Paolo, Astuto Marinella
Department of Anaesthesia and Intensive Care, "Policlinico-Vittorio Emanuele" University Hospital, 95123 Catania, Italy.
School of Anaesthesia and Intensive Care, University Hospital "G. Rodolico", University of Catania, 95123 Catania, Italy.
J Clin Med. 2021 Aug 31;10(17):3943. doi: 10.3390/jcm10173943.
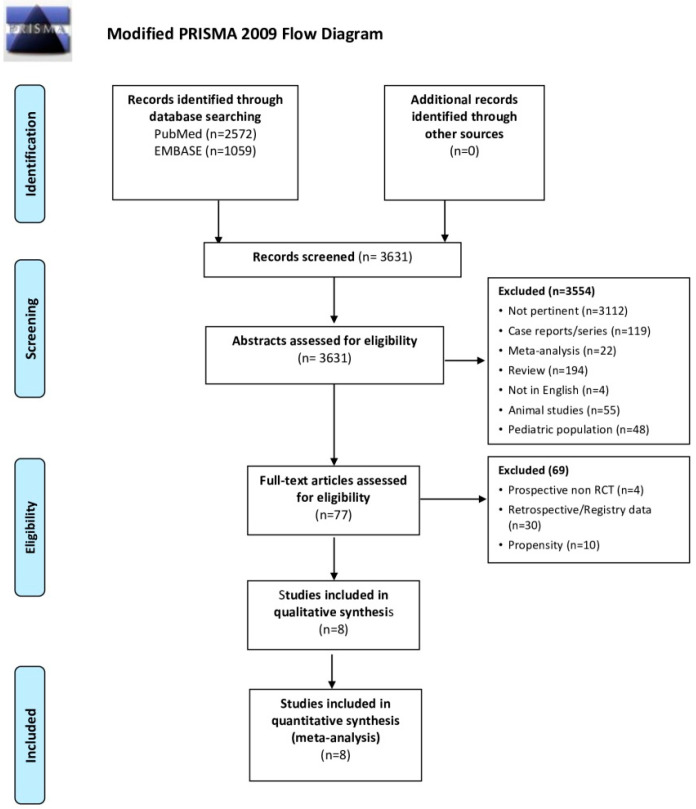
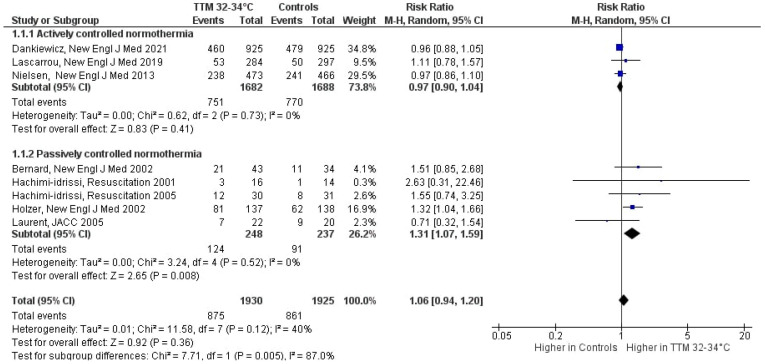
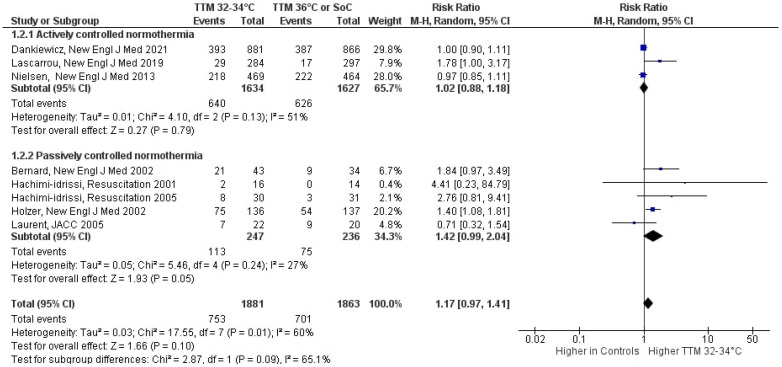
Target temperature management (TTM) in cardiac arrest (CA) survivors is recommended after hospital admission for its possible beneficial effects on survival and neurological outcome. Whether a lower target temperature (i.e., 32-34 °C) improves outcomes is unclear. We conducted a systematic review and meta-analysis on Pubmed and EMBASE to evaluate the effects on mortality and neurologic outcome of TTM at 32-34 °C as compared to controls (patients cared with "actively controlled" or "uncontrolled" normothermia). Results were analyzed via risk ratios (RR) and 95% confidence intervals (CI). Eight randomized controlled trials (RCTs) were included. TTM at 32-34 °C was compared to "actively controlled" normothermia in three RCTs and to "uncontrolled" normothermia in five RCTs. TTM at 32-34 °C does not improve survival as compared to normothermia (RR:1.06 (95%CI 0.94, 1.20), = 0.36; I = 39%). In the subgroup analyses, TTM at 32-34 °C is associated with better survival when compared to "uncontrolled" normothermia (RR: 1.31 (95%CI 1.07, 1.59), = 0.008) but shows no beneficial effects when compared to "actively controlled" normothermia (RR: 0.97 (95%CI 0.90, 1.04), = 0.41). TTM at 32-34 °C does not improve neurological outcome as compared to normothermia (RR: 1.17 (95%CI 0.97, 1.41), = 0.10; I = 60%). TTM at 32-34 °C increases the risk of arrhythmias (RR: 1.35 (95%CI 1.16, 1.57), = 0.0001, I = 0%). TTM at 32-34 °C does not improve survival nor neurological outcome after CA and increases the risk of arrhythmias.
心脏骤停(CA)幸存者入院后建议进行目标温度管理(TTM),因为其可能对生存和神经功能结局产生有益影响。较低的目标温度(即32-34°C)是否能改善结局尚不清楚。我们在PubMed和EMBASE上进行了一项系统评价和荟萃分析,以评估与对照组(接受“积极控制”或“未控制”正常体温治疗的患者)相比,32-34°C的TTM对死亡率和神经功能结局的影响。通过风险比(RR)和95%置信区间(CI)分析结果。纳入了八项随机对照试验(RCT)。在三项RCT中,将32-34°C的TTM与“积极控制”的正常体温进行比较,在五项RCT中与“未控制”的正常体温进行比较。与正常体温相比,32-34°C的TTM并不能提高生存率(RR:1.06(95%CI 0.94,1.20),P = 0.36;I² = 39%)。在亚组分析中,与“未控制”的正常体温相比,32-34°C的TTM与更好的生存率相关(RR:1.31(95%CI 1.07,1.59),P = 0.008),但与“积极控制”的正常体温相比没有有益效果(RR:0.97(95%CI 0.90,1.04)),P = 0.41)。与正常体温相比,32-34°C的TTM不能改善神经功能结局(RR:1.17(95%CI 0.97,1.41),P = 0.10;I² = 60%)。32-34°C的TTM会增加心律失常的风险(RR:1.35(95%CI 1.16,1.57),P = 0.0001,I² = 0%)。32-34°C的TTM不能改善心脏骤停后的生存率和神经功能结局,反而会增加心律失常的风险。