Lipid Peroxidation Unit, Laboratory of Clinical Investigation, National Institute on Aging, Baltimore, MD, USA
Intramural Program of the National Institute on Alcohol Abuse and Alcoholism, NIH, Bethesda, MD, USA.
BMJ. 2021 Jun 30;374:n1448. doi: 10.1136/bmj.n1448.
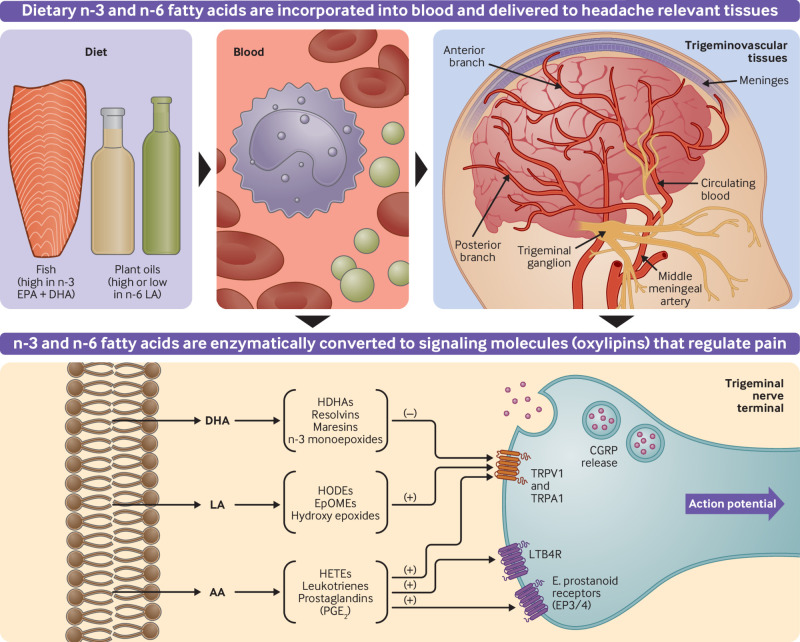
To determine whether dietary interventions that increase n-3 fatty acids with and without reduction in n-6 linoleic acid can alter circulating lipid mediators implicated in headache pathogenesis, and decrease headache in adults with migraine.
Three arm, parallel group, randomized, modified double blind, controlled trial.
Ambulatory, academic medical center in the United States over 16 weeks.
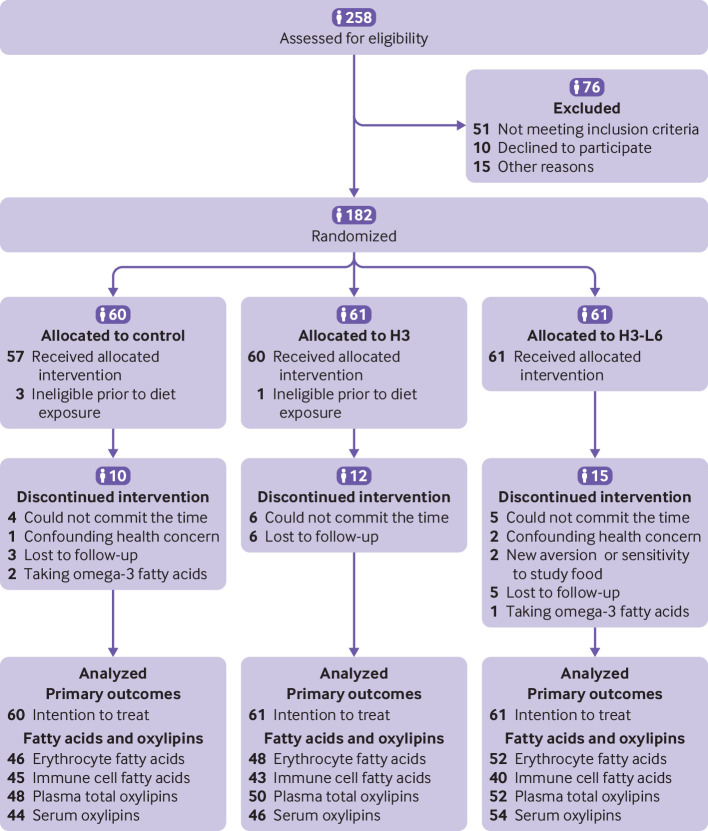
182 participants (88% women, mean age 38 years) with migraines on 5-20 days per month (67% met criteria for chronic migraine).
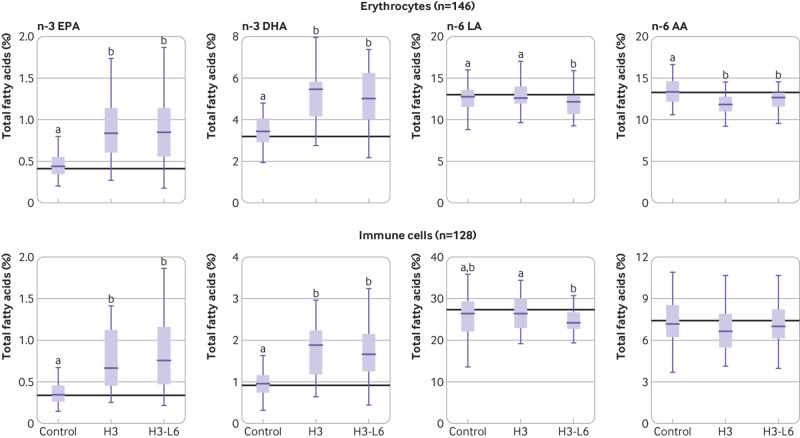
Three diets designed with eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and linoleic acid altered as controlled variables: H3 diet (n=61)-increase EPA+DHA to 1.5 g/day and maintain linoleic acid at around 7% of energy; H3-L6 diet (n=61)-increase n-3 EPA+DHA to 1.5 g/day and decrease linoleic acid to ≤1.8% of energy; control diet (n=60)-maintain EPA+DHA at <150 mg/day and linoleic acid at around 7% of energy. All participants received foods accounting for two thirds of daily food energy and continued usual care.
The primary endpoints (week 16) were the antinociceptive mediator 17-hydroxydocosahexaenoic acid (17-HDHA) in blood and the headache impact test (HIT-6), a six item questionnaire assessing headache impact on quality of life. Headache frequency was assessed daily with an electronic diary.
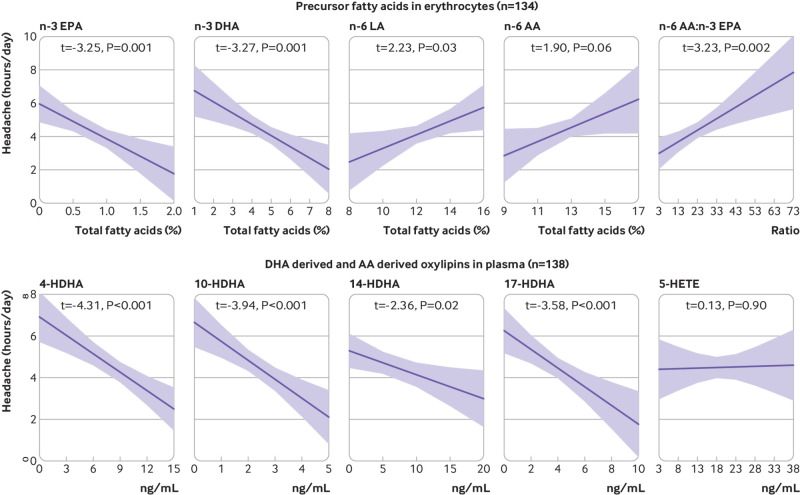
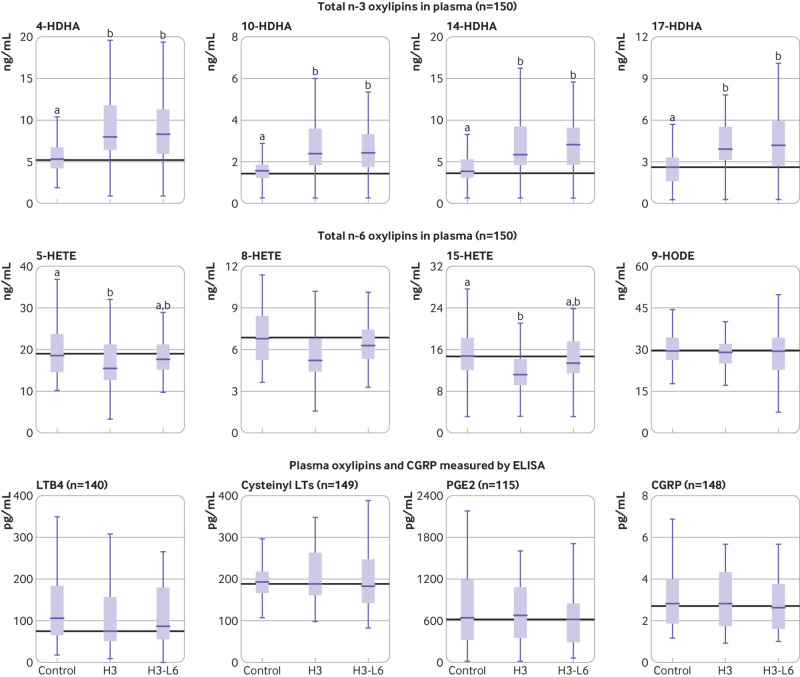
In intention-to-treat analyses (n=182), the H3-L6 and H3 diets increased circulating 17-HDHA (log ng/mL) compared with the control diet (baseline-adjusted mean difference 0.6, 95% confidence interval 0.2 to 0.9; 0.7, 0.4 to 1.1, respectively). The observed improvement in HIT-6 scores in the H3-L6 and H3 groups was not statistically significant (-1.6, -4.2 to 1.0, and -1.5, -4.2 to 1.2, respectively). Compared with the control diet, the H3-L6 and H3 diets decreased total headache hours per day (-1.7, -2.5 to -0.9, and -1.3, -2.1 to -0.5, respectively), moderate to severe headache hours per day (-0.8, -1.2 to -0.4, and -0.7, -1.1 to -0.3, respectively), and headache days per month (-4.0, -5.2 to -2.7, and -2.0, -3.3 to -0.7, respectively). The H3-L6 diet decreased headache days per month more than the H3 diet (-2.0, -3.2 to -0.8), suggesting additional benefit from lowering dietary linoleic acid. The H3-L6 and H3 diets altered n-3 and n-6 fatty acids and several of their nociceptive oxylipin derivatives in plasma, serum, erythrocytes or immune cells, but did not alter classic headache mediators calcitonin gene related peptide and prostaglandin E2.
The H3-L6 and H3 interventions altered bioactive mediators implicated in headache pathogenesis and decreased frequency and severity of headaches, but did not significantly improve quality of life.
ClinicalTrials.gov NCT02012790.
确定增加 n-3 脂肪酸并减少 n-6 亚油酸是否可以改变与头痛发病机制相关的循环脂质介质,并减少偏头痛成人的头痛。
三臂、平行组、随机、改良双盲、对照试验。
美国门诊、学术医疗中心,持续 16 周。
182 名偏头痛患者(88%为女性,平均年龄 38 岁),每月头痛 5-20 天(67%符合慢性偏头痛标准)。
三种设计的饮食含有二十碳五烯酸(EPA)、二十二碳六烯酸(DHA)和亚油酸作为控制变量:H3 饮食(n=61)-增加 EPA+DHA 至 1.5 克/天,维持亚油酸在能量的 7%左右;H3-L6 饮食(n=61)-增加 n-3 EPA+DHA 至 1.5 克/天,将亚油酸减少至能量的≤1.8%;对照饮食(n=60)-维持 EPA+DHA 低于 150mg/天,亚油酸维持在能量的 7%左右。所有参与者均接受占每日食物能量三分之二的食物,并继续常规护理。
主要终点(第 16 周)为血液中的镇痛介质 17-羟二十二碳六烯酸(17-HDHA)和头痛影响测试(HIT-6),这是一个评估头痛对生活质量影响的六项问卷。每日使用电子日记评估头痛频率。
意向治疗分析(n=182)中,H3-L6 和 H3 饮食与对照饮食相比,增加了循环 17-HDHA(logng/mL)(基线调整平均差异 0.6,95%置信区间 0.2 至 0.9;0.7,0.4 至 1.1)。H3-L6 和 H3 组 HIT-6 评分的改善不具有统计学意义(-1.6,-4.2 至 1.0;-1.5,-4.2 至 1.2)。与对照饮食相比,H3-L6 和 H3 饮食减少了每日总头痛时间(-1.7,-2.5 至-0.9;-1.3,-2.1 至-0.5)、中度至重度头痛时间(-0.8,-1.2 至-0.4;-0.7,-1.1 至-0.3)和每月头痛天数(-4.0,-5.2 至-2.7;-2.0,-3.3 至-0.7)。H3-L6 饮食减少每月头痛天数比 H3 饮食更多(-2.0,-3.2 至-0.8),表明降低饮食中亚油酸可带来额外的益处。H3-L6 和 H3 饮食改变了 n-3 和 n-6 脂肪酸及其在血浆、血清、红细胞或免疫细胞中的几种疼痛敏化氧合脂衍生物,但没有改变经典的头痛介质降钙素基因相关肽和前列腺素 E2。
H3-L6 和 H3 干预措施改变了与头痛发病机制相关的生物活性介质,并减少了头痛的频率和严重程度,但对生活质量没有显著改善。
ClinicalTrials.gov NCT02012790。