Department of Emergency Medicine, University of Florida College of Medicine - Jacksonville, 655 West 8th Street, Jacksonville, FL, 32209, USA.
Center for Data Solutions, University of Florida College of Medicine - Jacksonville, Jacksonville, FL, USA.
Crit Care. 2021 Sep 17;25(1):341. doi: 10.1186/s13054-021-03757-5.
Approximately one-third of sepsis patients experience poor outcomes including chronic critical illness (CCI, intensive care unit (ICU) stay > 14 days) or early death (in-hospital death within 14 days). We sought to characterize lipoprotein predictive ability for poor outcomes and contribution to sepsis heterogeneity.
Prospective cohort study with independent replication cohort.
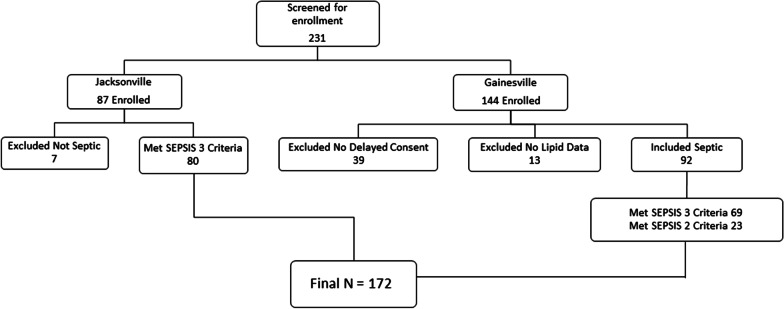
Emergency department and surgical ICU at two hospitals.
Sepsis patients presenting within 24 h.
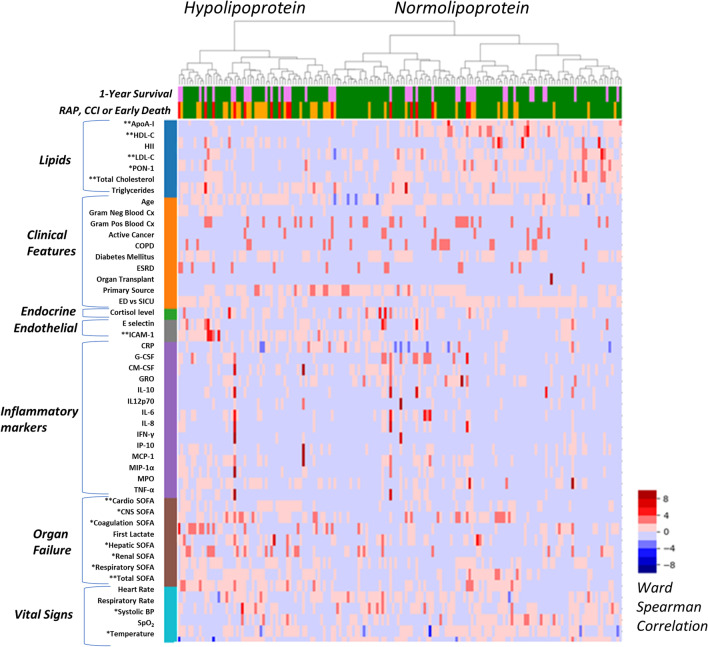
Measures included cholesterol levels (total cholesterol, high density lipoprotein cholesterol [HDL-C], low density lipoprotein cholesterol [LDL-C]), triglycerides, paraoxonase-1 (PON-1), and apolipoprotein A-I (Apo A-I) in the first 24 h. Inflammatory and endothelial markers, and sequential organ failure assessment (SOFA) scores were also measured. LASSO selection assessed predictive ability for outcomes. Unsupervised clustering was used to investigate the contribution of lipid variation to sepsis heterogeneity.
172 patients were enrolled. Most (~ 67%, 114/172) rapidly recovered, while ~ 23% (41/172) developed CCI, and ~ 10% (17/172) had early death. ApoA-I, LDL-C, mechanical ventilation, vasopressor use, and Charlson Comorbidity Score were significant predictors of CCI/early death in LASSO models. Unsupervised clustering yielded two discernible phenotypes. The Hypolipoprotein phenotype was characterized by lower lipoprotein levels, increased endothelial dysfunction (ICAM-1), higher SOFA scores, and worse clinical outcomes (45% rapid recovery, 40% CCI, 16% early death; 28-day mortality, 21%). The Normolipoprotein cluster patients had higher cholesterol levels, less endothelial dysfunction, lower SOFA scores and better outcomes (79% rapid recovery, 15% CCI, 6% early death; 28-day mortality, 15%). Phenotypes were validated in an independent replication cohort (N = 86) with greater sepsis severity, which similarly demonstrated lower HDL-C, ApoA-I, and higher ICAM-1 in the Hypolipoprotein cluster and worse outcomes (46% rapid recovery, 23% CCI, 31% early death; 28-day mortality, 42%). Normolipoprotein patients in the replication cohort had better outcomes (55% rapid recovery, 32% CCI, 13% early death; 28-day mortality, 28%) Top features for cluster discrimination were HDL-C, ApoA-I, total SOFA score, total cholesterol level, and ICAM-1.
Lipoproteins predicted poor sepsis outcomes. A Hypolipoprotein sepsis phenotype was identified and characterized by lower lipoprotein levels, increased endothelial dysfunction (ICAM-1) and organ failure, and worse clinical outcomes.
大约三分之一的脓毒症患者预后不良,包括慢性危重病(CCI,入住重症监护病房[ICU]超过 14 天)或早期死亡(住院 14 天内死亡)。我们旨在描述脂蛋白对不良预后的预测能力及其对脓毒症异质性的贡献。
前瞻性队列研究和独立复制队列。
两家医院的急诊科和外科重症监护病房。
脓毒症患者在 24 小时内就诊。
在最初 24 小时内测量胆固醇水平(总胆固醇、高密度脂蛋白胆固醇[HDL-C]、低密度脂蛋白胆固醇[LDL-C])、甘油三酯、对氧磷酶-1(PON-1)和载脂蛋白 A-I(Apo A-I)。还测量了炎症和内皮标记物以及序贯器官衰竭评估(SOFA)评分。LASSO 选择评估了对结果的预测能力。无监督聚类用于研究脂质变化对脓毒症异质性的贡献。
共纳入 172 例患者。大多数(~67%,114/172)迅速康复,而约 23%(41/172)发生 CCI,约 10%(17/172)早期死亡。ApoA-I、LDL-C、机械通气、血管加压素使用和 Charlson 合并症评分是 LASSO 模型中 CCI/早期死亡的显著预测因子。无监督聚类产生了两种可区分的表型。低脂蛋白表型的特征是脂蛋白水平较低,内皮功能障碍增加(ICAM-1),SOFA 评分较高,临床结局较差(45%快速恢复,40%CCI,16%早期死亡;28 天死亡率,21%)。载脂蛋白 A-I 和更高的 SOFA 评分以及更好的结果(79%快速恢复,15%CCI,6%早期死亡;28 天死亡率,15%)。表型在独立的复制队列(N=86)中得到验证,该队列的脓毒症严重程度更高,低脂蛋白表型的 HDL-C、ApoA-I 和 ICAM-1 水平更低,预后更差(46%快速恢复,23%CCI,31%早期死亡;28 天死亡率,42%)。复制队列中载脂蛋白 A-I 的低脂蛋白患者的预后更好(55%快速恢复,32%CCI,13%早期死亡;28 天死亡率,28%)。聚类判别特征是 HDL-C、ApoA-I、总 SOFA 评分、总胆固醇水平和 ICAM-1。
脂蛋白预测脓毒症不良预后。确定并描述了一种低脂蛋白脓毒症表型,其特征是脂蛋白水平较低、内皮功能障碍(ICAM-1)增加和器官衰竭以及临床结局较差。