Yu Bin, Akushevich Igor, Yashkin Arseniy P, Kravchenko Julia
Department of Surgery, School of Medicine, Duke University, Durham, NC, United States.
Social Science Research Institute, Duke University, Durham, NC, United States.
Front Cardiovasc Med. 2021 Sep 9;8:707102. doi: 10.3389/fcvm.2021.707102. eCollection 2021.
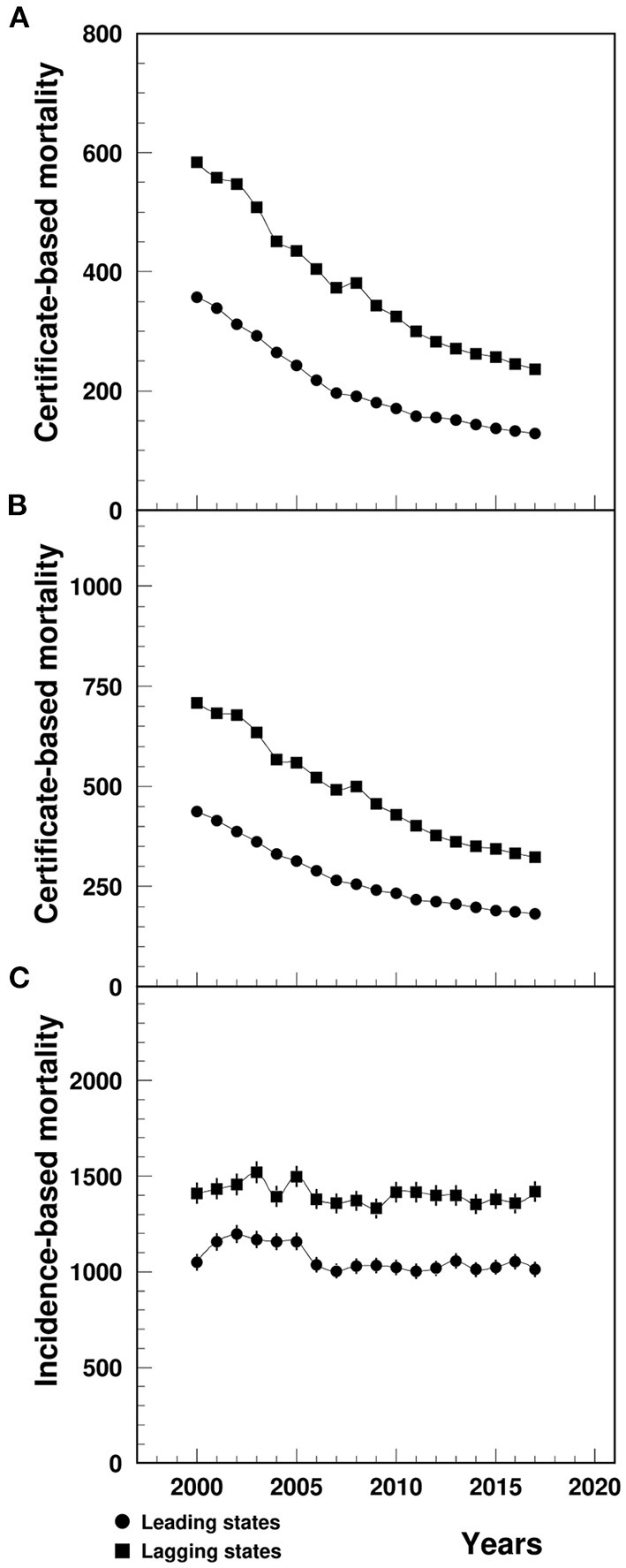
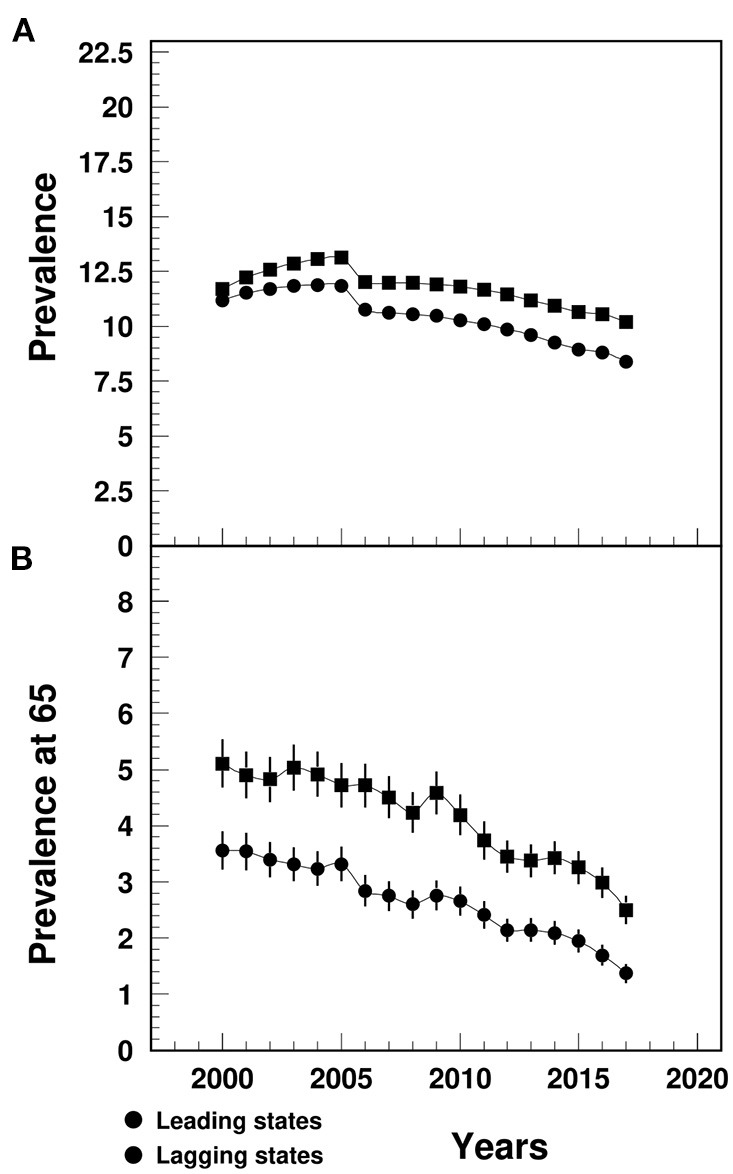
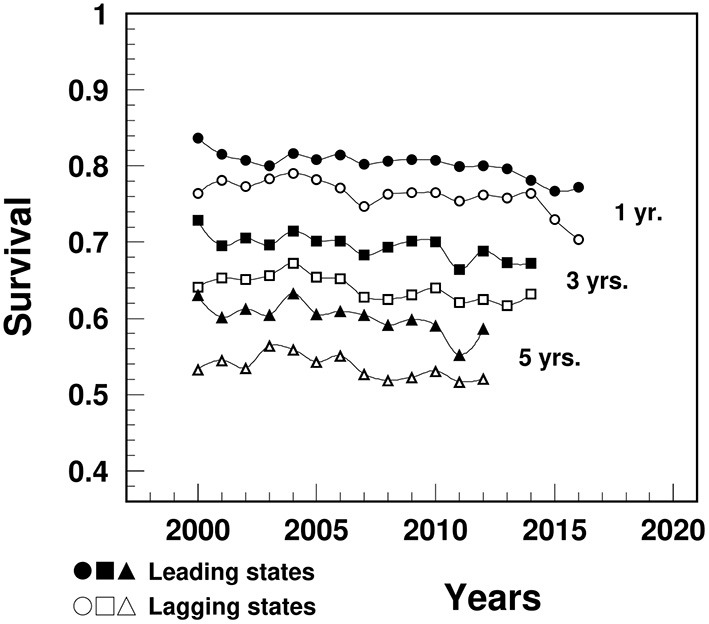
There are substantial geographic disparities in the life expectancy (LE) across the U.S. with myocardial infarction (MI) contributing significantly to the differences between the states with highest (leading) and lowest (lagging) LE. This study aimed to systematically investigate the epidemiology of geographic disparities in MI among older adults. Data on MI outcomes among adults aged 65+ were derived from the Center for Disease Control and Prevention-sponsored Wide-Ranging Online Data for Epidemiologic Research database and a 5% sample of Medicare Beneficiaries for 2000-2017. Death certificate-based mortality from MI as underlying/multiple cause of death (CBM-UCD/CBM-MCD), incidence-based mortality (IBM), incidence, prevalence, prevalence at age 65, and 1-, 3-, and 5-year survival, and remaining LE at age 65 were estimated and compared between the leading and lagging states. Cox model was used to investigate the effect of residence in the lagging states on MI incidence and survival. Between 2000 and 2017, MI mortality was higher in the lagging than in the leading states (per 100,000, CBM-UCD: 236.7-583.7 vs. 128.2-357.6, CBM-MCD: 322.7-707.7 vs. 182.4-437.7, IBM: 1330.5-1518.9 vs. 1003.3-1197.0). Compared to the leading states, lagging states had higher MI incidence (1.1-2.0% vs. 0.9-1.8%), prevalence (10.2-13.1% vs. 8.3-11.9%), pre-existing prevalence (2.5-5.1% vs. 1.4-3.6%), and lower survival (70.4 vs. 77.2% for 1-year, 63.2 vs. 67.2% for 3-year, and 52.1 vs. 58.7% for 5-year), and lower remaining LE at age 65 among MI patients (years, 8.8-10.9 vs. 9.9-12.8). Cox model results showed that the lagging states had greater risk of MI incidence [Adjusted hazards ratio, AHR (95% Confidence Interval, CI): 1.18 (1.16, 1.19)] and death after MI diagnosis [1.22 (1.21, 1.24)]. Study results also showed alarming declines in survival and remaining LE at age 65 among MI patients. There are substantial geographic disparities in MI outcomes, with lagging states having higher MI mortality, incidence, and prevalence, lower survival and remaining LE at age 65. Disparities in MI mortality in a great extent could be due to between-the-state differences in MI incidence, prevalence at age 65 and survival. Observed declines in survival and remaining LE require an urgent analysis of contributing factors that must be addressed.
美国各地的预期寿命(LE)存在显著的地理差异,心肌梗死(MI)在预期寿命最高(领先)和最低(滞后)的州之间的差异中起了重要作用。本研究旨在系统调查老年人中MI地理差异的流行病学情况。65岁及以上成年人的MI结局数据来自疾病控制和预防中心资助的广泛在线流行病学研究数据库以及2000 - 2017年医疗保险受益人的5%样本。基于死亡证明的MI作为潜在/多种死因的死亡率(CBM - UCD/CBM - MCD)、基于发病率的死亡率(IBM)、发病率、患病率、65岁时的患病率以及1年、3年和5年生存率,以及65岁时的剩余预期寿命,在领先州和滞后州之间进行了估计和比较。使用Cox模型研究居住在滞后州对MI发病率和生存率的影响。在2000年至2017年期间,滞后州的MI死亡率高于领先州(每10万人,CBM - UCD:236.7 - 583.7对128.2 - 357.6,CBM - MCD:322.7 - 707.7对182.4 - 437.7,IBM:1330.5 - 1518.9对1003.3 - 1197.0)。与领先州相比,滞后州的MI发病率更高(1.1 - 2.0%对0.9 - 1.8%)、患病率更高(10.2 - 13.1%对8.3 - 11.9%)、既往患病率更高(2.5 - 5.1%对1.4 - 3.6%),生存率更低(1年时为70.4%对77.2%,3年时为63.2%对67.2%,5年时为52.1%对58.7%),并且MI患者65岁时的剩余预期寿命更低(年数,8.8 - 10.9对9.9 - 12.8)。Cox模型结果显示,滞后州发生MI的风险更大[调整后风险比,AHR(95%置信区间,CI):1.18(1.16,1.19)],MI诊断后死亡的风险更大[1.22(1.21,1.24)]。研究结果还显示,MI患者65岁时的生存率和剩余预期寿命出现了惊人的下降。MI结局存在显著的地理差异,滞后州的MI死亡率、发病率和患病率更高,65岁时的生存率和剩余预期寿命更低。MI死亡率的差异在很大程度上可能归因于各州之间MI发病率、65岁时的患病率和生存率的差异。观察到的生存率和剩余预期寿命的下降需要对必须解决的促成因素进行紧急分析。