University of Minnesota School of Public Health, Minneapolis.
Division of General Internal Medicine and Health Services Research, David Geffen School of Medicine at UCLA, Los Angeles, California.
JAMA Netw Open. 2019 Mar 1;2(3):e190634. doi: 10.1001/jamanetworkopen.2019.0634.
The Medicare Hospital Readmissions Reduction Program (HRRP) has disproportionately penalized hospitals that treat many black patients, which could worsen health outcomes in this population.
To determine whether short-term mortality rates increased among black and white adults 65 years and older after initiation of the HRRP and whether trends differed by race.
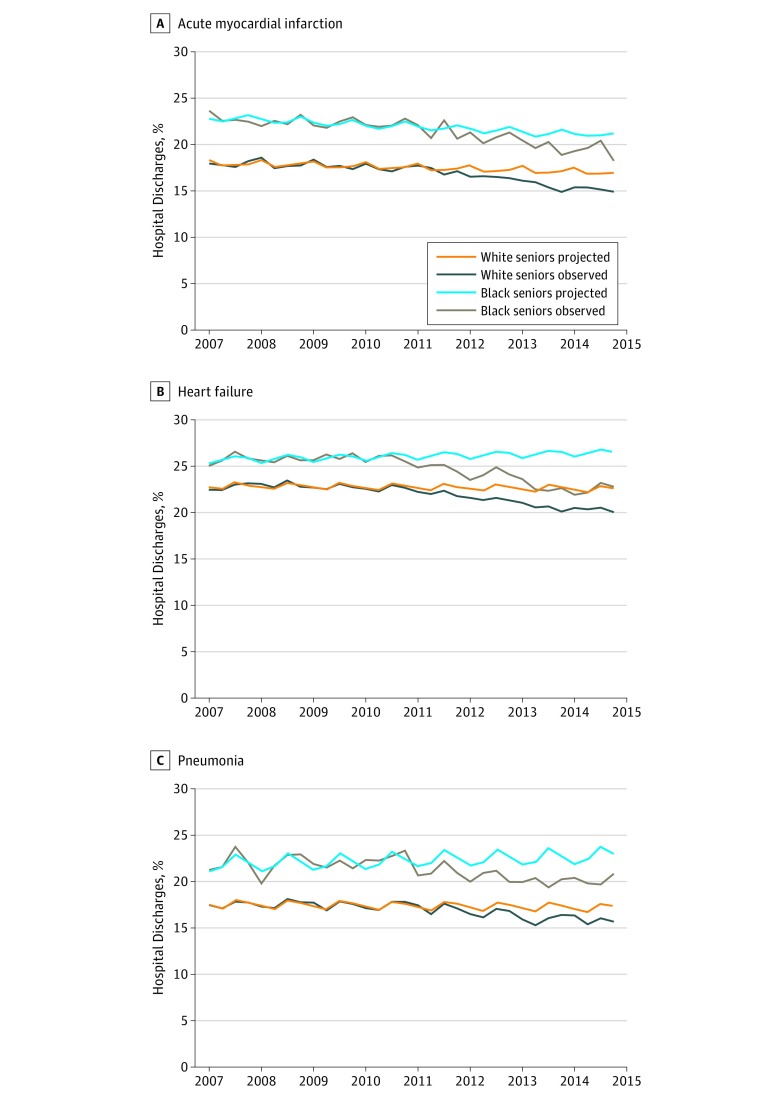
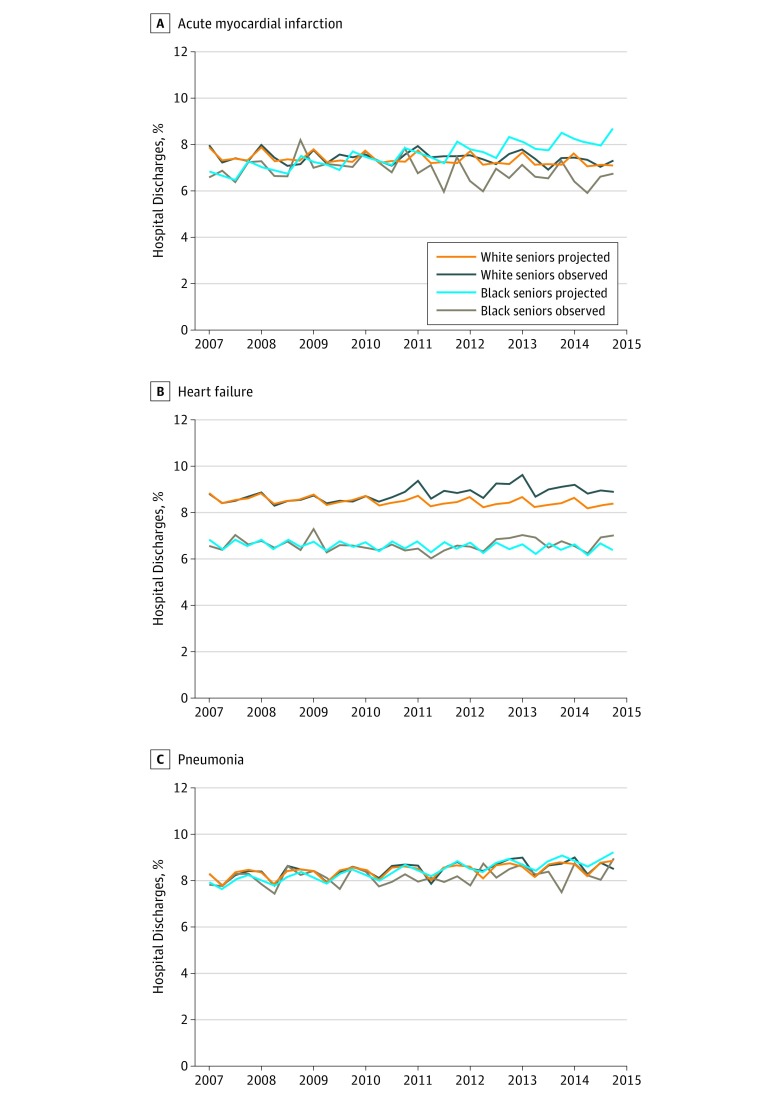
DESIGN, SETTING, AND PARTICIPANTS: In a cohort study using an interrupted time-series analysis conducted from March 15, 2018, to January 23, 2019, in 3263 eligible acute care hospitals nationally, risk-adjusted mortality rates observed after Medicare started to impose penalties (October 1, 2012, to November 30, 2014) were compared with projections based on pre-HRRP trends (January 1, 2007, to March 31, 2010) among adults 65 years and older with acute myocardial infarction (AMI), heart failure (HF), or pneumonia. Observed-to-projected differences were then compared between racial groups.
Hospital discharge during pre-HRRP and HRRP penalty periods.
Thirty-day postdischarge all-cause mortality.
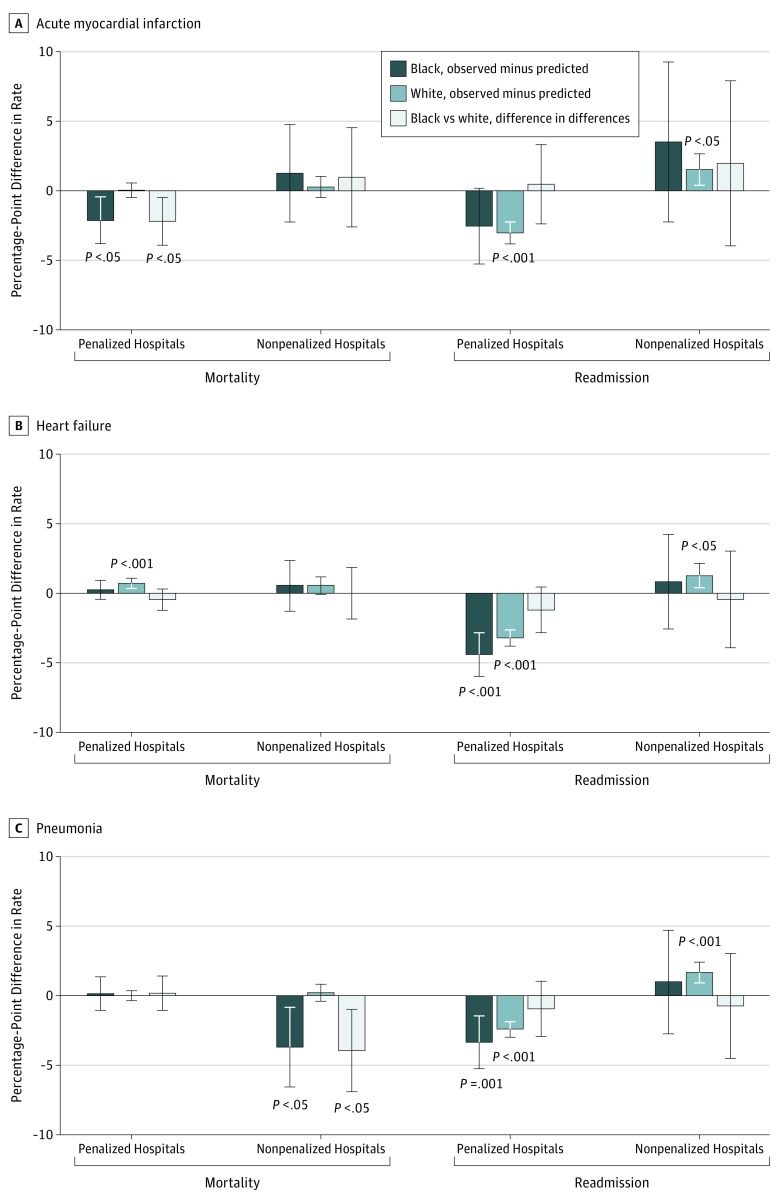
In the 3263 acute care hospitals included in the analysis, black patients (627 373 index discharges) were more likely than white patients (5 845 130 index discharges) to be younger (mean [SD] age, 77.8 [8.3] vs 80.5 [8.2] years; P < .001), women (60.5% vs 53.7%; P < .001), dually covered by Medicare and Medicaid (45.7% vs 17.2%; P < .001), and treated at a penalized hospital (AMI, 82.8%; HF, 83.8%; and pneumonia, 82.6% vs 69.6%; 73.3%; and 71.7%; all P < .001). Pre-HRRP mortality rates for black vs white patients were 7.04% (95% CI, 6.75% to 7.33%) vs 7.47% (95% CI, 7.37% to 7.57%) for AMI, 6.69% (95% CI, 6.56% to 6.82%) vs 8.56% (95% CI, 8.48% to 8.64%) for HF, and 8.08% (95% CI, 7.88% to 8.27%) vs 8.27% (95% CI, 8.19% to 8.35%) for pneumonia. By the HRRP penalty period, observed mortality for AMI decreased more, relative to projections, among black than white patients (difference-in-differences, -1.65 percentage points; 95% CI, -3.19 to -0.10; P = .04). For HF, mortality increased relative to projections among white patients but not among black patients; however; mortality trends did not differ by race (difference-in-differences, -0.37 percentage points; 95% CI, -1.08 to 0.34; P = .31). For pneumonia, observed mortality was similar to projections in both racial groups, and trends did not differ by race (difference-in-differences, -0.54 percentage points; 95% CI, -1.66 to 0.59; P = .35). At both penalized and nonpenalized hospitals, mortality trends were similar or decreased more among black patients than white patients.
In this study of patients 65 years and older, short-term postdischarge mortality did not appear to increase for black patients under the HRRP, suggesting that certain value-based payment policies can be implemented without harming black populations. However, mortality seemed to increase for white patients with HF and this situation warrants investigation.
医疗保险医院再入院减少计划(HRRP)不成比例地惩罚了治疗许多黑人员工的医院,这可能会恶化该人群的健康结果。
确定在 HRRP 启动后,65 岁及以上的黑人和白人成年人的短期死亡率是否增加,以及种族之间的趋势是否存在差异。
设计、设置和参与者:在一项使用中断时间序列分析的队列研究中,从 2018 年 3 月 15 日至 2019 年 1 月 23 日,在全国 3263 家符合条件的急性护理医院中,对 Medicare 开始实施处罚(2012 年 10 月 1 日至 2014 年 11 月 30 日)后观察到的死亡率与基于 HRRP 前趋势(2007 年 1 月 1 日至 2010 年 3 月 31 日)的预测进行了比较,在年龄为 65 岁及以上的急性心肌梗死(AMI)、心力衰竭(HF)或肺炎患者中。然后比较了两个种族群体之间观察到的差异与预测值之间的差异。
HRRP 处罚期和 HRRP 处罚期前的医院出院。
30 天的全因死亡率。
在分析中纳入的 3263 家急性护理医院中,黑人员工(627373 次指数出院)比白人员工(5845130 次指数出院)更年轻(平均[SD]年龄,77.8[8.3]岁 vs 80.5[8.2]岁;P<.001),女性(60.5% vs 53.7%;P<.001),同时由医疗保险和医疗补助覆盖(45.7% vs 17.2%;P<.001),并且在受处罚的医院接受治疗(AMI,82.8%;HF,83.8%;和肺炎,82.6% vs 69.6%;73.3%;和 71.7%;均 P<.001)。与白人患者相比,黑人患者的 HRRP 前死亡率为 7.04%(95%CI,6.75%至 7.33%) vs 7.47%(95%CI,7.37%至 7.57%),AMI;6.69%(95%CI,6.56%至 6.82%) vs 8.56%(95%CI,8.48%至 8.64%),HF;8.08%(95%CI,7.88%至 8.27%) vs 8.27%(95%CI,8.19%至 8.35%),肺炎。在 HRRP 处罚期间,与预测值相比,AMI 患者的死亡率下降幅度更大,黑人患者比白人患者差异为-1.65%(95%CI,-3.19 至-0.10;P=.04)。对于 HF,白人患者的死亡率相对于预测值有所上升,但黑人患者的死亡率没有上升;然而,死亡率趋势在种族之间没有差异(差异,-0.37%;95%CI,-1.08 至 0.34;P=.31)。对于肺炎,两个种族组的观察死亡率与预测值相似,趋势在种族之间没有差异(差异,-0.54%;95%CI,-1.66 至 0.59;P=.35)。在受处罚和不受处罚的医院中,黑人患者的死亡率趋势与白人患者相似或下降更多。
在这项针对 65 岁及以上患者的研究中,HRRP 下黑人患者的短期出院后死亡率似乎没有增加,这表明某些基于价值的支付政策可以实施而不会对黑人造成伤害。然而,HF 患者的死亡率似乎有所上升,这种情况需要进一步调查。