Department of Dental Implant Center, Beijing Stomatological Hospital, School of Stomatology, Capital Medical University, No. 4 Tian Tan Xi Li, Dongcheng District, Beijing, 100050, People's Republic of China.
BMC Oral Health. 2021 Sep 27;21(1):476. doi: 10.1186/s12903-021-01843-2.
Restoration with locking-taper implants is a widely used methodology. However, conical connection systems such as locking-taper implant systems have rarely been examined. This study provides a retrospective investigation of locking-taper fixed restorations, mainly focusing on prosthetic complications.
Patients undergo treatment with conical connected implants from 2008 to 2010 were examined. Preparation of the implant sites was performed according to the standard procedures for the Bicon system. Bone healing took over 6 months, and the prosthetic procedure was initiated thereafter. Integrated abutment crowns or gold porcelain crowns were used, and the prosthesis type was a single crown or a fixed dental prosthesis. Once the crown was in place, its occlusion was thoroughly checked and adjusted, and then the crown was glazed or finely polished. The Kaplan-Meier method was used to calculate the cumulative complication-free rates for 5 and 10 years. Additionally, a Cox regression model was used to identify the factors that independently influenced the results. Implant survival and marginal bone loss were also investigated.
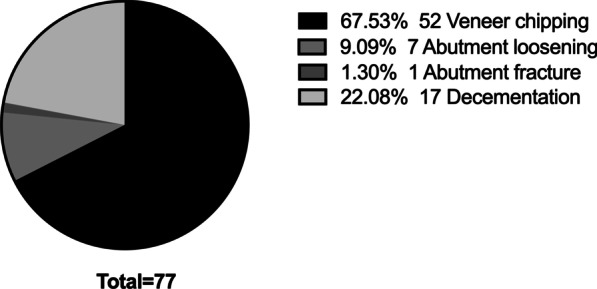
A total of 392 patients who underwent 541 implants and 434 locking taper implant-based restorations from 2008 to 2010 were examined. The overall 5-year cumulative complication-free rate was 83.34%. The most common prosthetic complication was veneer chipping, with a frequency of 67.53%. According to the Cox regression model, the complication-free rate of integrated abutment crowns was significantly higher than that of gold porcelain crowns, that of molar regions was significantly higher than that of premolar regions, and that of females was significantly higher than that of males. Only three implant failures happened, and the mean marginal bone loss values at 1- year, 5-years and 10- years were 0.25 mm (95% CI ± 0.12), 0.40 mm (95% CI ± 0.03) and 0.51 mm (95% CI ± 0.05), respectively.
Veneer chipping was the most common complication with locking-taper implant-supported fixed restorations. The incidence of complications for IACs is significantly higher than that for GPCs. Age, location, and prosthesis type are not determinants of prosthetic complications. Besides, the long-term clinical effect of locking-taper implant can meet the clinical needs. The bone tissue level around the implant can maintain long-term stability.
采用锁定锥形种植体进行修复是一种广泛应用的方法。然而,对于锥形连接系统,如锁定锥形种植体系统,研究却相对较少。本研究对锁定锥形固定修复体进行了回顾性调查,主要关注修复体并发症。
对 2008 年至 2010 年间采用锥形连接种植体进行治疗的患者进行了检查。种植体部位的准备按照 Bicon 系统的标准程序进行。骨愈合时间超过 6 个月,然后开始进行修复程序。采用整体基台冠或金瓷冠,修复体类型为单冠或固定义齿。牙冠就位后,对其咬合进行彻底检查和调整,然后对牙冠进行上釉或精细抛光。采用 Kaplan-Meier 法计算 5 年和 10 年的无并发症累积率。此外,还使用 Cox 回归模型来确定独立影响结果的因素。还对种植体的存活率和边缘骨丧失进行了研究。
共检查了 2008 年至 2010 年间接受 541 枚种植体和 434 枚基于锁定锥形种植体修复体的 392 名患者。总体 5 年无并发症累积率为 83.34%。最常见的修复体并发症是贴面碎裂,发生率为 67.53%。根据 Cox 回归模型,整体基台冠的无并发症率明显高于金瓷冠,磨牙区明显高于前磨牙区,女性明显高于男性。只有 3 例种植体失败,种植体 1 年、5 年和 10 年时的平均边缘骨丧失值分别为 0.25mm(95%置信区间±0.12)、0.40mm(95%置信区间±0.03)和 0.51mm(95%置信区间±0.05)。
贴面碎裂是锁定锥形种植体支持固定修复体最常见的并发症。IAC 的并发症发生率明显高于 GPC。年龄、位置和修复体类型不是修复体并发症的决定因素。此外,锁定锥形种植体的长期临床效果能够满足临床需求。种植体周围的骨组织水平能够保持长期稳定。