Section for Nutrition Research, Department of Metabolism, Digestion and Reproduction, Faculty of Medicine, Imperial College London, London, UK.
Section of Endocrinology and Investigative Medicine, Department of Metabolism, Digestion and Reproduction, Faculty of Medicine, Imperial College London, London, UK.
J Cachexia Sarcopenia Muscle. 2021 Dec;12(6):2134-2144. doi: 10.1002/jcsm.12820. Epub 2021 Sep 29.
Skeletal muscle mass begins to decline from 40 years of age. Limited data suggest that dietary fibre may modify lean body mass (BM), of which skeletal muscle is the largest and most malleable component. We investigated the relationship between dietary fibre intake, skeletal muscle mass and associated metabolic and functional parameters in adults aged 40 years and older.
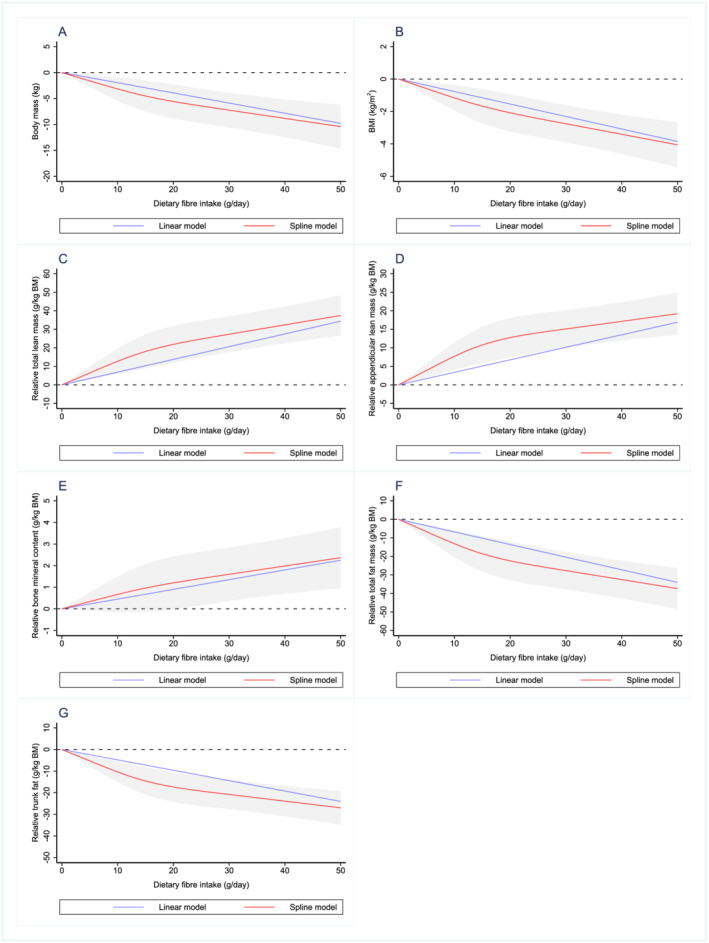
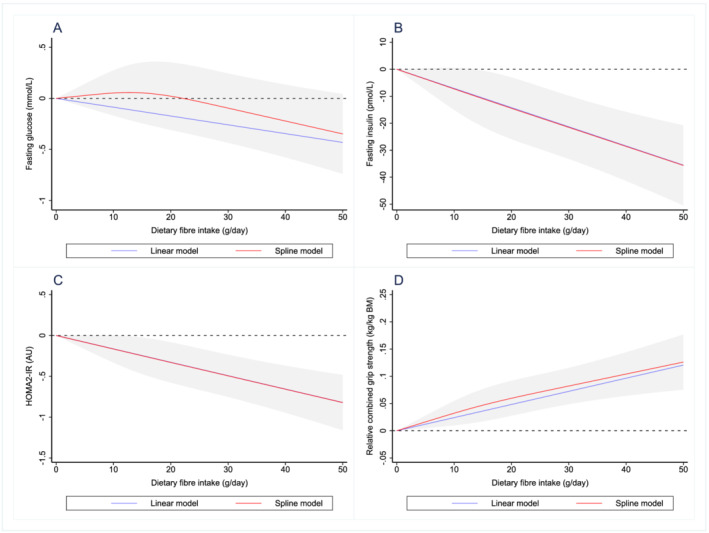
We analysed cross-sectional data from the US National Health and Nutrition Examination Survey between 2011 and 2018 from adults aged 40 years and older. Covariate-adjusted multiple linear regression analyses were used to evaluate the association between dietary fibre intake and BM components (BM, body mass index [BMI], total lean mass, appendicular lean mass, bone mineral content, total fat, trunk fat; n = 6454), glucose homeostasis (fasting glucose, fasting insulin, HOMA2-IR; n = 5032) and skeletal muscle strength (combined grip strength; n = 5326). BM components and skeletal muscle strength were expressed relative to BM (per kg of BM).
Higher intakes of dietary fibre were significantly associated with increased relative total lean mass (β: 0.69 g/kg BM; 95% CI, 0.48-0.89 g/kg BM; P < 0.001), relative appendicular lean mass (β: 0.34 g/kg BM; 95% CI, 0.23-0.45 g/kg BM; P < 0.001), relative bone mineral content (β: 0.05 g/kg BM; 95% CI, 0.02-0.07 g/kg BM; P < 0.001) and relative combined grip strength (β: 0.002 kg/kg BM; 95% CI, 0.001-0.003 kg/kg BM; P < 0.001). Conversely, higher dietary fibre intakes were significantly associated with a lower BM (β: -0.20; 95% CI, -0.28 to -0.11 kg; P < 0.001), BMI (β: -0.08 kg/m ; 95%CI, -0.10 to -0.05 kg/m ), relative total fat (β: -0.68 g/kg BM; 95% CI, -0.89 to -0.47 g/kg BM; P < 0.001), relative trunk fat (β: -0.48 g/kg BM; 95%CI, -0.63 to -0.33 g/kg; P < 0.001), fasting glucose (β: -0.01 mmol/L; 95% CI, -0.02 to -0.00 mmol/L; P = 0.017), fasting insulin (β: -0.71 pmol/L; 95% CI, -1.01 to -0.41 pmol/L; P < 0.001) and HOMA2-IR (β: -0.02 AU; 95% CI, -0.02 to -0.01 AU; P < 0.001).
Higher dietary fibre intakes are associated with a lower BM and enhanced body composition, characterized by a reduction in fat mass and an increase in lean mass. Higher dietary fibre intakes were also associated with improvements in glucose homeostasis and skeletal muscle strength. Increasing dietary fibre intake may be a viable strategy to prevent age-associated declines in skeletal muscle mass.
从 40 岁开始,骨骼肌量开始下降。有限的数据表明,膳食纤维可能会改变瘦体重(BM),其中骨骼肌是最大和最具可塑性的成分。我们研究了 40 岁及以上成年人膳食纤维摄入量与骨骼肌量及相关代谢和功能参数之间的关系。
我们分析了 2011 年至 2018 年期间美国国家健康和营养检查调查的横断面数据,纳入 40 岁及以上成年人。采用协变量调整的多元线性回归分析评估膳食纤维摄入量与 BM 成分(BM、体重指数[BMI]、总瘦体重、四肢瘦体重、骨矿物质含量、总脂肪、躯干脂肪;n=6454)、葡萄糖稳态(空腹血糖、空腹胰岛素、HOMA2-IR;n=5032)和骨骼肌力量(握力总和;n=5326)之间的关系。BM 成分和骨骼肌力量相对于 BM(每公斤 BM)进行表示。
较高的膳食纤维摄入量与相对总瘦体重增加显著相关(β:0.69g/kg BM;95%置信区间,0.48-0.89 g/kg BM;P<0.001)、相对四肢瘦体重增加(β:0.34 g/kg BM;95%置信区间,0.23-0.45 g/kg BM;P<0.001)、相对骨矿物质含量增加(β:0.05 g/kg BM;95%置信区间,0.02-0.07 g/kg BM;P<0.001)和相对握力总和增加(β:0.002 kg/kg BM;95%置信区间,0.001-0.003 kg/kg BM;P<0.001)。相反,较高的膳食纤维摄入量与 BM 降低显著相关(β:-0.20;95%置信区间,-0.28 至-0.11 kg;P<0.001)、BMI 降低(β:-0.08 kg/m;95%置信区间,-0.10 至-0.05 kg/m)、相对总脂肪降低(β:-0.68 g/kg BM;95%置信区间,-0.89 至-0.47 g/kg BM;P<0.001)、相对躯干脂肪降低(β:-0.48 g/kg BM;95%置信区间,-0.63 至-0.33 g/kg;P<0.001)、空腹血糖降低(β:-0.01 mmol/L;95%置信区间,-0.02 至-0.00 mmol/L;P=0.017)、空腹胰岛素降低(β:-0.71 pmol/L;95%置信区间,-1.01 至-0.41 pmol/L;P<0.001)和 HOMA2-IR 降低(β:-0.02 AU;95%置信区间,-0.02 至-0.01 AU;P<0.001)。
较高的膳食纤维摄入量与 BM 降低和身体成分改善有关,表现为脂肪量减少和瘦体重增加。较高的膳食纤维摄入量也与葡萄糖稳态和骨骼肌力量的改善有关。增加膳食纤维摄入量可能是预防与年龄相关的骨骼肌量下降的可行策略。