Sehgal Tushar, Gupta Nitesh, Kohli Santvana, Khurana Aditi, Dass Jasmita, Diwan Sahil, A J Mahendran, Khan Maroof, Aggarwal Mukul, Subramanian Arulselvi
Laboratory Medicine, All India Institute of Medical Sciences, New Delhi, IND.
Internal Medicine • Pulmonology, Vardhman Mahavir Medical College, Safdarjung Hospital, New Delhi, IND.
Cureus. 2021 Aug 26;13(8):e17463. doi: 10.7759/cureus.17463. eCollection 2021 Aug.
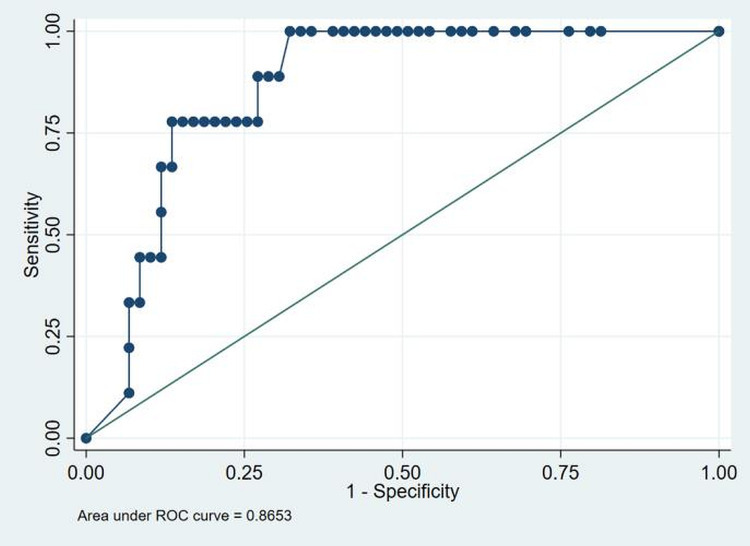
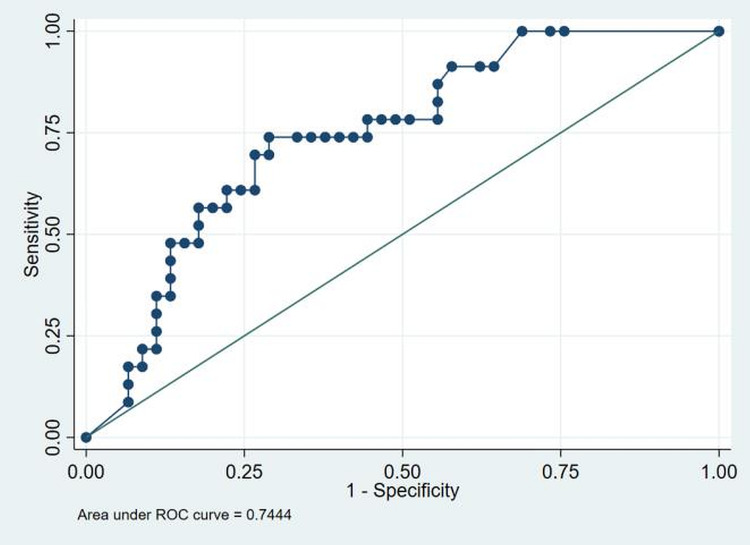
Background Acute respiratory distress syndrome (ARDS) is a frequent complication of COVID-19 and is associated with a component of thrombo-inflammation and cytokine storm. COVID-19 also affects the hemostatic system causing multiple coagulation abnormalities that is a cause of concern and needs to be addressed. Objective We aimed to assess coagulation parameters of COVID-19 patients and identify whether they could be used as potential prognostic biomarkers to predict ARDS and immediate outcomes. Methods This was a prospective study done on 68 patients at four serial time points. Patients between 18-85 years admitted to the hospital as in-patients and ICU with a confirmed diagnosis of COVID-19 by RT-PCR were included. Exclusion criteria included pregnancy, patients below and above the mentioned age, previously known coagulopathy, systemic anticoagulants or anti-platelet therapy or vitamin K antagonists and moribund patients. Patients were divided into three categories based on SOFA score at admission, presence (group 1) or absence (group 2) of ARDS and outcome (dead or alive). Routine and specialized coagulation tests were performed on patients' platelet-poor plasma at the time of study inclusion (day 0), days 3, 7 and at discharge on STAR Max®3 (Diagnostica Stago France) automated coagulation analyzer and included prothrombin time (PT), international normalized ratio (INR) (STA® -NeoPTimal), activated partial thromboplastin time (APTT) (STA® -Cephascreen), fibrinogen (STA® Liquid Fib), D-dimer (STA® LiatestD- Dimer), Protein C (STA Stachrom® Protein C), Protein S (STA® Latest Free Protein S) and Antithrombin (STA® Chrom ATIII). ELISA did testing for tissue plasminogen activator (Asserachrom® tPA) as per the manufacturer's protocol. Results Sixty-eight patients, including 43 (63%) males and 25 (37%) females, with a median age of 48 years (IQR 20-85), were recruited in this study. The incidence of ARDS was 34%, with a mortality of 13%. History of contact with a COVID-19 case was present in 71% (48/68) of the patients. Fever was the most common presenting symptom in 84% (57/68) of the patients. The most common comorbidities were hypertension and diabetes mellitus (DM) in 22% (15/68) and 21% (14/68) of the patients. DM (p=0.07) and chronic obstructive pulmonary disease (COPD) (p=0.03) were significantly associated with ARDS. DM (p=0.02), hypertension (p=0.01), and COPD (p=0.02) were also significantly associated with mortality. APTT was markedly prolonged among non-survivors at day 0 (D0) and D7 (p=0.03, p=0.02). D-Dimer was elevated in 38/68 (56%) patients at D0. D-Dimer levels were significantly higher in non-survivors (p<0.001), in ARDS patients (p=0.001) and patients with higher SOFA scores (p=0.001). ROC curve showed that D-dimer cut-off > 2.13 (AUC of 0.86) and >0.85 (AUC of 0.74) predicts mortality and ARDS, respectively. Among the natural anticoagulants, protein C was significantly associated with a high SOFA score at D0 and D3 (p=0.04). Conclusion Diabetes mellitus, hypertension and COPD were associated with poor outcomes. D-dimer levels must be monitored in COVID patients due to their association with ARDS and mortality. We observed that the levels of natural anticoagulants fell during the illness, making them prone to coagulopathies; however, none were seen in this study. Elevated tPA levels were also found in our patients; fibrinolytic therapy may benefit COVID-19 patients suffering from ARDS.
背景 急性呼吸窘迫综合征(ARDS)是新型冠状病毒肺炎(COVID-19)的常见并发症,与血栓炎症和细胞因子风暴有关。COVID-19还会影响止血系统,导致多种凝血异常,这令人担忧且需要解决。 目的 我们旨在评估COVID-19患者的凝血参数,并确定它们是否可作为预测ARDS和近期预后的潜在预后生物标志物。 方法 这是一项对68例患者在四个连续时间点进行的前瞻性研究。纳入年龄在18 - 85岁之间、因确诊COVID-19而住院和入住重症监护病房(ICU)的患者。排除标准包括妊娠、上述年龄范围之外的患者、既往已知的凝血病、全身抗凝或抗血小板治疗或维生素K拮抗剂以及濒死患者。根据入院时的序贯器官衰竭评估(SOFA)评分、ARDS的存在(第1组)或不存在(第2组)以及预后(死亡或存活)将患者分为三类。在研究纳入时(第0天)、第3天、第7天以及出院时,使用STAR Max®3(法国Diagnostica Stago公司)自动凝血分析仪对患者的乏血小板血浆进行常规和特殊凝血检测,检测项目包括凝血酶原时间(PT)、国际标准化比值(INR)(STA® -NeoPTimal)、活化部分凝血活酶时间(APTT)(STA® -Cephascreen)、纤维蛋白原(STA® Liquid Fib)、D-二聚体(STA® LiatestD-Dimer)、蛋白C(STA Stachrom® Protein C)、蛋白S(STA® Latest Free Protein S)和抗凝血酶(STA® Chrom ATIII)。根据制造商的方案,采用酶联免疫吸附测定(ELISA)检测组织型纤溶酶原激活剂(Asserachrom® tPA)。 结果 本研究共招募了68例患者,其中男性43例(63%),女性25例(37%),中位年龄为48岁(四分位间距20 - 85岁)。ARDS的发生率为34%,死亡率为13%。71%(48/68)的患者有COVID-19病例接触史。发热是84%(57/68)患者最常见的首发症状。最常见的合并症是高血压和糖尿病,分别占患者的22%(15/68)和21%(14/68)。糖尿病(p = 0.07)和慢性阻塞性肺疾病(COPD)(p = 0.03)与ARDS显著相关。糖尿病(p = 0.02)、高血压(p = 0.01)和COPD(p = 0.02)也与死亡率显著相关。在第0天(D0)和第7天,非幸存者的APTT明显延长(p = 0.03,p = 0.02)。在D0时,38/68(56%)的患者D-二聚体升高。非幸存者(p < 0.001)、ARDS患者(p = 0.001)和SOFA评分较高的患者(p = 0.001)的D-二聚体水平显著更高。ROC曲线显示,D-二聚体临界值> 2.13(曲线下面积[AUC]为0.86)和> 0.85(AUC为0.74)分别预测死亡率和ARDS。在天然抗凝剂中,蛋白C在D0和D3时与高SOFA评分显著相关(p = 0.04)。 结论 糖尿病、高血压和COPD与不良预后相关。由于D-二聚体水平与ARDS和死亡率相关,因此必须对COVID患者进行监测。我们观察到,在疾病期间天然抗凝剂水平下降,使患者易于发生凝血病;然而,本研究中未观察到这种情况。我们的患者中还发现tPA水平升高;纤维蛋白溶解疗法可能使患有ARDS的COVID-19患者受益。