Kagimoto Atsushi, Tsutani Yasuhiro, Kambara Takahiro, Handa Yoshinori, Kumada Takashi, Mimae Takahiro, Kushitani Kei, Miyata Yoshihiro, Takeshima Yukio, Okada Morihito
Department of Surgical Oncology, Hiroshima University, Kasumi, Hiroshima, Japan.
Department of Pathology, Hiroshima University, Kasumi, Hiroshima, Japan.
JTO Clin Res Rep. 2020 Nov 26;2(2):100126. doi: 10.1016/j.jtocrr.2020.100126. eCollection 2021 Feb.
The International Association for the Study of Lung Cancer proposed a new grading criteria for invasive adenocarcinoma. However, its utility has not been validated.
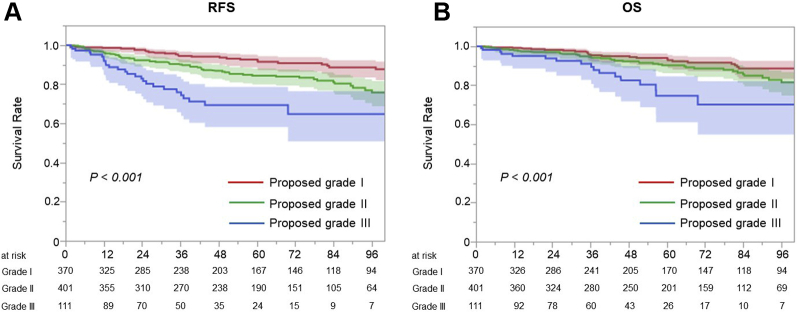
Patients who underwent complete resection of lung adenocarcinoma were included in this study. Then, they were divided into the following three groups on the basis of the criteria recently proposed by the International Association for the Study of Lung Cancer: grade 1, lepidic predominant tumor, with less than 20% of high-grade patterns; grade 2, acinar or papillary predominant tumor, with less than 20% of high-grade patterns; and grade 3, any tumor with greater than or equal to 20% of high-grade patterns.
Recurrence-free survival (RFS) was significantly different among the proposed grades ( < 0.001). The RFS of patients upgrading from current grade 2 (papillary or acinar predominant tumor) to proposed grade 3 (5-y RFS, 65.2%) was significantly worse than that of patients with proposed grade 2 (77.1%, hazard ratio = 1.882, 95% confidence interval: 1.236-2.866) but not significantly different from that of patients with grade 3 in both the current (micropapillary or solid predominant tumor) and proposed criteria (53.2%, hazard ratio = 0.761, 95% confidence interval: 0.456-1.269). Among patients with pathologic stage 0 or I, RFS was well stratified by the new grading system ( < 0.001) but not among patients with stage II or III ( = 0.334). In the multivariable analysis, the new grading was not a predictive factor of RFS.
Although the proposed grading system well stratified RFS in patients with pathologic stage 0 or I lung adenocarcinoma, there is room for improvement.
国际肺癌研究协会提出了一种新的浸润性腺癌分级标准。然而,其效用尚未得到验证。
本研究纳入了接受肺腺癌完全切除的患者。然后,根据国际肺癌研究协会最近提出的标准,将他们分为以下三组:1级,以鳞屑状为主的肿瘤,高级别模式占比小于20%;2级,以腺泡或乳头状为主的肿瘤,高级别模式占比小于20%;3级,高级别模式占比大于或等于20%的任何肿瘤。
在提议的分级中,无复发生存期(RFS)有显著差异(<0.001)。从当前2级(乳头状或腺泡状为主的肿瘤)升级到提议的3级(5年RFS,65.2%)的患者的RFS明显差于提议2级的患者(77.1%,风险比=1.882,95%置信区间:1.236-2.866),但与当前(微乳头状或实性为主的肿瘤)和提议标准中3级患者(53.2%)无显著差异(风险比=0.761,95%置信区间:0.456-1.269)。在病理分期为0或I期的患者中,新的分级系统能很好地对RFS进行分层(<0.001),但在II期或III期患者中则不然(=0.334)。在多变量分析中,新分级不是RFS的预测因素。
尽管提议的分级系统能很好地对病理分期为0或I期肺腺癌患者的RFS进行分层,但仍有改进空间。