Cottereau Guillaume, Messika Jonathan, Megarbane Bruno, Guérin Laurent, da Silva Daniel, Bornstain Caroline, Santos Matilde, Ricard Jean-Damien, Sztrymf Benjamin
AP-HP, Service de Rééducation Fonctionnelle et Kinésithérapie, Hôpital Antoine Béclère, 92140, Clamart, France.
AP-HP, Hôpital Louis Mourier, DMU ESPRIT, Service de Médecine Intensive Réanimation, Université de Paris, 92700, Colombes, France.
Ann Intensive Care. 2021 Oct 2;11(1):144. doi: 10.1186/s13613-021-00932-3.
ICU-acquired weakness (ICUAW) has been shown to be associated with prolonged duration of mechanical ventilation and extubation failure. It is usually assessed through Medical Research Council (MRC) score, a time-consuming score performed by physiotherapists. Handgrip strength (HG) can be monitored very easily at the bedside. It has been shown to be a reproducible and reliable marker of global muscular strength in critical care patients. We sought to test if muscular weakness, as assessed by handgrip strength, was associated with extubation outcome.
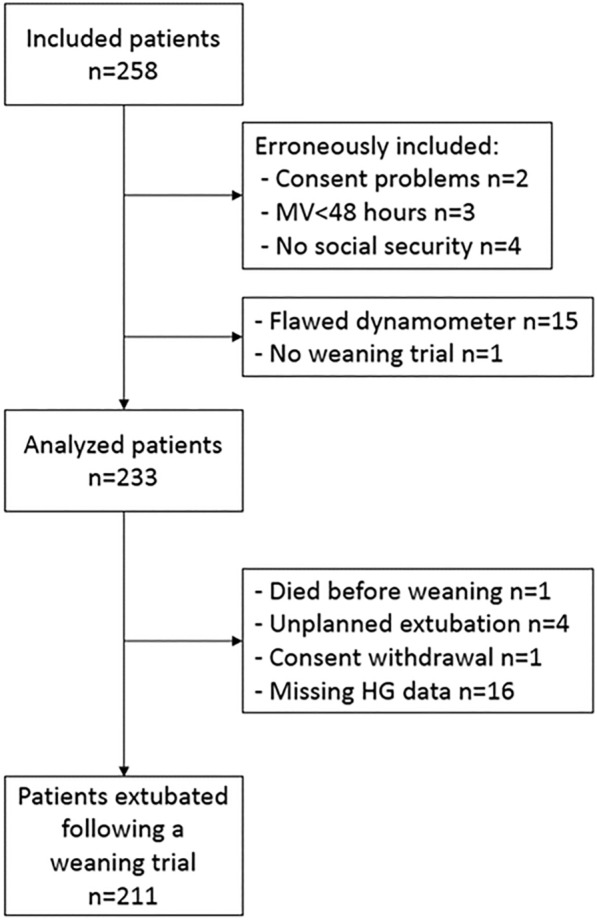
Prospective multicenter trial over an 18 months period in six mixed ICUs. Adults receiving mechanical ventilation for at least 48 h were eligible. Just before weaning trial, HG, Maximal Inspiratory Pressure (MIP), Peak Cough Expiratory Flow (PCEF) and Medical Research Council (MRC) score were registered. The attending physicians were unaware of the tests results and weaning procedures were conducted according to guidelines. Occurrence of unscheduled reintubation, non-invasive ventilation (NIV) or high-flow nasal continuous oxygen (HFNC) because of respiratory failure within 7 days after extubation defined extubation failure. The main outcome was the link between HG and extubation outcome.
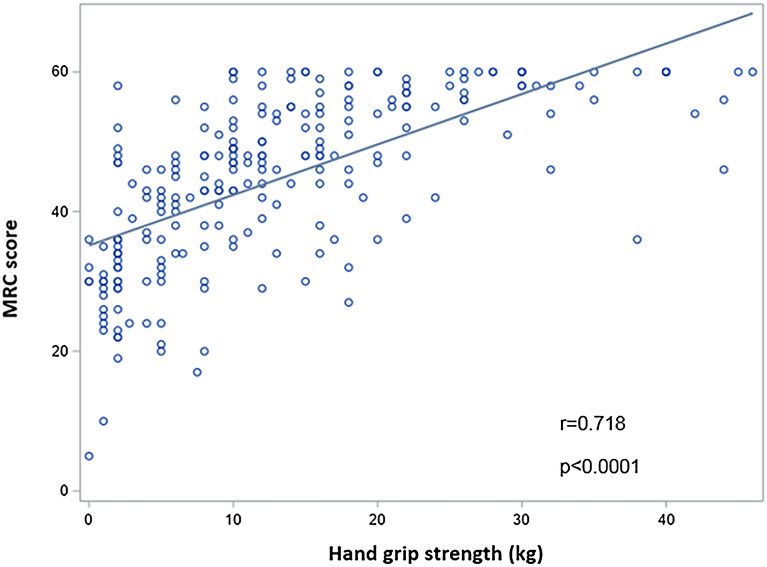
233 patients were included. Extubation failure occurred in 51 (22.5%) patients, 39 (17.2%) required reintubation. Handgrip strength was 12 [6-20] kg and 12 [8-20] kg, respectively, in extubation success and failure (p = 0.85). There was no association between extubation outcome and MRC score, MIP or PCEF. Handgrip strength was well correlated with MRC score (r = 0.718, p < 0.0001). ICU and hospital length of stay were significantly higher in the subset of patients harboring muscular weakness as defined by handgrip performed at the first weaning trial (respectively, 15 [10-25] days vs. 11 [7-17] days, p = 0.001 and 34 [19-66] days vs. 22 [15-43] days, p = 0.002).
No association was found between handgrip strength and extubation outcome. Whether this was explained by the appropriateness of the tool in this specific setting, or by the precise impact of ICUAW on extubation outcome deserves to be further evaluated. Trial registration Clinical Trials; NCT02946502, 10/27/2016, URL: https://clinicaltrials.gov/ct2/results?cond=&term=gripwean&cntry=&state=&city=&dist=.
重症监护病房获得性肌无力(ICUAW)已被证明与机械通气时间延长和拔管失败有关。它通常通过医学研究委员会(MRC)评分来评估,这是一项由物理治疗师进行的耗时评分。握力(HG)可以在床边非常容易地进行监测。它已被证明是危重症患者整体肌肉力量的可重复且可靠的指标。我们试图测试通过握力评估的肌肉无力是否与拔管结果相关。
在6个综合性重症监护病房进行了为期18个月的前瞻性多中心试验。接受机械通气至少48小时的成年人符合条件。在撤机试验前,记录握力、最大吸气压力(MIP)、咳嗽峰值呼气流量(PCEF)和医学研究委员会(MRC)评分。主治医生不知道测试结果,撤机程序按照指南进行。拔管后7天内因呼吸衰竭发生计划外重新插管、无创通气(NIV)或高流量鼻持续给氧(HFNC)定义为拔管失败。主要结果是握力与拔管结果之间的联系。
纳入233例患者。51例(22.5%)患者发生拔管失败,39例(17.2%)需要重新插管。拔管成功和失败患者的握力分别为12[6 - 20]kg和12[8 - 20]kg(p = 0.85)。拔管结果与MRC评分、MIP或PCEF之间无关联。握力与MRC评分密切相关(r = 0.718,p < 0.0001)。在首次撤机试验时通过握力定义为存在肌肉无力的患者亚组中,重症监护病房住院时间和住院时间显著更长(分别为15[10 - 25]天对11[7 - 17]天,p = 0.001;34[19 - 66]天对22[15 - 43]天,p = 0.002)。
未发现握力与拔管结果之间存在关联。这是由于该工具在这种特定情况下的适用性,还是由于ICUAW对拔管结果的确切影响,值得进一步评估。试验注册 临床试验;NCT02946502,2016年10月27日,网址:https://clinicaltrials.gov/ct2/results?cond=&term=gripwean&cntry=&state=&city=&dist= 。