Institute of Healthcare Management, Strathmore University Business School, Strathmore University, Nairobi, Kenya.
Department of Global Health and Development, London School of Hygiene and Tropical Medicine, University of London, London, UK.
Int J Health Policy Manag. 2022 Sep 1;11(9):1852-1862. doi: 10.34172/ijhpm.2021.90. Epub 2021 Aug 25.
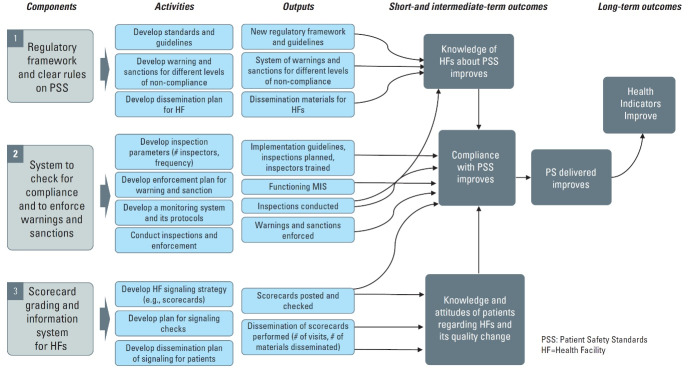
Health facility regulation in low- and middle-income countries (LMICs) is generally weak, with potentially serious consequences for safety and quality. Innovative regulatory reforms were piloted in three Kenyan counties including: a Joint Health Inspection Checklist (JHIC) synthesizing requirements across multiple regulatory agencies; increased inspection frequency; allocating facilities to compliance categories which determined warnings, sanctions and/or time to re-inspection; and public display of regulatory results. The reforms substantially increased inspection scores compared with control facilities. We developed lessons for future regulatory policy from this pilot by identifying key factors that facilitated or hindered its implementation.
We conducted a qualitative study to understand views and experiences of actors involved in the one-year pilot. We interviewed 77 purposively selected staff from the national, county and facility levels. Data were analyzed using the framework approach, identifying facilitating/hindering factors at the facility, inspection system, and health system levels.
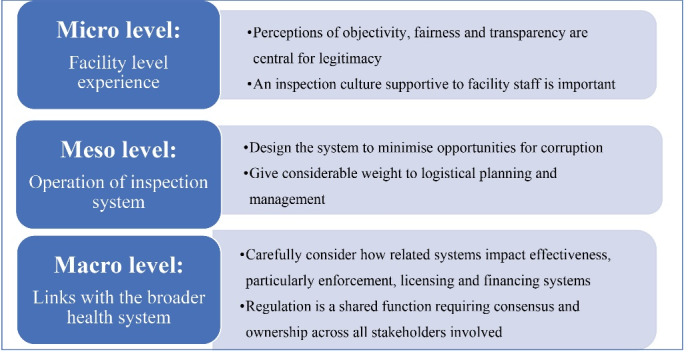
The joint health inspections (JHIs) were generally viewed as fair, objective and transparent, which enhanced their perceived legitimacy. Interactions with inspectors were described as friendly and supportive, in contrast to the punitive culture of previous inspections when bribery had been common. Inspector training and use of an electronic checklist were strongly praised. However, practical challenges with transport, route planning and budgets highlighted the critical nature of strong logistical management. The effectiveness of inspection in improving compliance was hampered by limitations in related systems, particularly facility licensing, enforcement of closures and, in the public sector, control of funds. However, an inclusive reform development process had led to high buy-in across regulatory agencies which was key to the system's success.
Effective facility inspection involves more than "hardware" such as checklists, protocols and training. Cultural, relational and institutional "software" are also crucial for legitimacy, feasibility of implementation and enforceability, and should be carefully integrated into regulatory reforms.
中低收入国家(LMICs)的卫生机构监管普遍薄弱,这可能对安全性和质量造成严重后果。在肯尼亚的三个县试点了创新性监管改革,包括:一个综合了多个监管机构要求的联合健康检查清单(JHIC);增加了检查频率;将设施分配到合规类别,确定警告、制裁和/或重新检查的时间;以及公开显示监管结果。与对照设施相比,这些改革使检查评分大幅提高。我们从试点中为未来的监管政策制定了经验教训,确定了促进或阻碍其实施的关键因素。
我们开展了一项定性研究,以了解参与为期一年试点的参与者的观点和经验。我们采访了来自国家、县和设施各级的 77 名有针对性选择的工作人员。使用框架方法分析数据,确定设施、检查系统和卫生系统各级的促进/阻碍因素。
联合健康检查(JHIs)通常被认为是公平、客观和透明的,这提高了它们的合法性。检查员与检查员的互动被描述为友好和支持的,与以前检查时的惩罚文化形成鲜明对比,当时贿赂很常见。检查员的培训和电子检查表的使用受到了强烈赞扬。然而,运输、路线规划和预算方面的实际挑战突显了强有力的后勤管理的重要性。与相关系统的限制,特别是设施许可、关闭的执行以及公共部门对资金的控制,限制了检查在提高合规性方面的有效性。然而,包容性的改革发展过程导致了监管机构的高度认同,这是该系统成功的关键。
有效的设施检查不仅仅涉及检查表、协议和培训等“硬件”。文化、关系和制度“软件”对于合法性、实施可行性和可执行性也至关重要,应谨慎纳入监管改革。