Krembil Centre for Neuroinformatics, Centre for Addiction and Mental Health, Toronto, Canada.
Institute for Molecular Medicine Finland (FIMM), University of Helsinki, Helsinki, Finland.
PLoS Med. 2021 Oct 12;18(10):e1003782. doi: 10.1371/journal.pmed.1003782. eCollection 2021 Oct.
Sleep problems are both symptoms of and modifiable risk factors for many psychiatric disorders. Wrist-worn accelerometers enable objective measurement of sleep at scale. Here, we aimed to examine the association of accelerometer-derived sleep measures with psychiatric diagnoses and polygenic risk scores in a large community-based cohort.
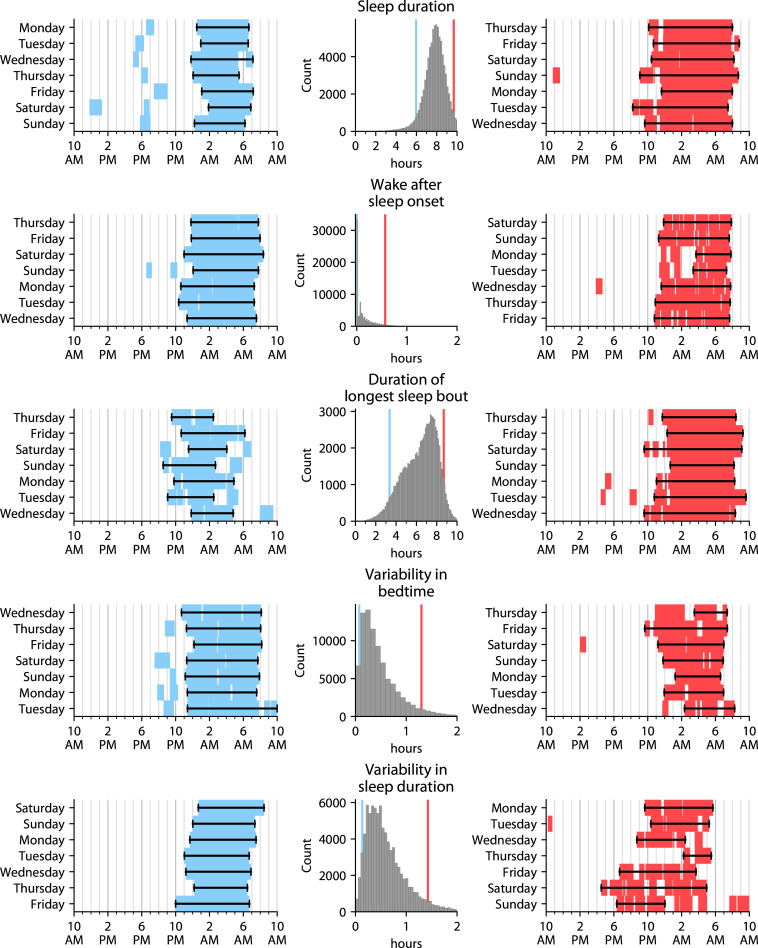
In this post hoc cross-sectional analysis of the UK Biobank cohort, 10 interpretable sleep measures-bedtime, wake-up time, sleep duration, wake after sleep onset, sleep efficiency, number of awakenings, duration of longest sleep bout, number of naps, and variability in bedtime and sleep duration-were derived from 7-day accelerometry recordings across 89,205 participants (aged 43 to 79, 56% female, 97% self-reported white) taken between 2013 and 2015. These measures were examined for association with lifetime inpatient diagnoses of major depressive disorder, anxiety disorders, bipolar disorder/mania, and schizophrenia spectrum disorders from any time before the date of accelerometry, as well as polygenic risk scores for major depression, bipolar disorder, and schizophrenia. Covariates consisted of age and season at the time of the accelerometry recording, sex, Townsend deprivation index (an indicator of socioeconomic status), and the top 10 genotype principal components. We found that sleep pattern differences were ubiquitous across diagnoses: each diagnosis was associated with a median of 8.5 of the 10 accelerometer-derived sleep measures, with measures of sleep quality (for instance, sleep efficiency) generally more affected than mere sleep duration. Effect sizes were generally small: for instance, the largest magnitude effect size across the 4 diagnoses was β = -0.11 (95% confidence interval -0.13 to -0.10, p = 3 × 10-56, FDR = 6 × 10-55) for the association between lifetime inpatient major depressive disorder diagnosis and sleep efficiency. Associations largely replicated across ancestries and sexes, and accelerometry-derived measures were concordant with self-reported sleep properties. Limitations include the use of accelerometer-based sleep measurement and the time lag between psychiatric diagnoses and accelerometry.
In this study, we observed that sleep pattern differences are a transdiagnostic feature of individuals with lifetime mental illness, suggesting that they should be considered regardless of diagnosis. Accelerometry provides a scalable way to objectively measure sleep properties in psychiatric clinical research and practice, even across tens of thousands of individuals.
睡眠问题既是许多精神疾病的症状,也是可改变的风险因素。腕戴式加速计可大规模实现睡眠的客观测量。在此,我们旨在检查在大型基于社区的队列中,加速计衍生的睡眠测量与精神疾病诊断和多基因风险评分之间的关联。
在 UK Biobank 队列的这项事后横断面分析中,从 89205 名参与者(年龄 43 至 79 岁,56%为女性,97%自我报告为白人)在 2013 年至 2015 年期间进行的 7 天加速计记录中得出了 10 种可解释的睡眠测量值-就寝时间,醒来时间,睡眠时间,睡眠后醒来,睡眠效率,醒来次数,最长睡眠时间,打盹次数以及就寝时间和睡眠时间的变化。这些措施与从加速计日期之前的任何时间开始的主要抑郁障碍,焦虑症,双相情感障碍/躁狂症和精神分裂症谱系障碍的终生住院诊断以及主要抑郁症,双相情感障碍和精神分裂症的多基因风险评分进行了关联。协变量包括加速计记录时的年龄和季节,性别,汤森剥夺指数(社会经济地位的指标)以及前 10 个基因型主成分。我们发现,睡眠模式差异在所有诊断中都普遍存在:每种诊断均与 10 个加速计衍生的睡眠测量中的中位数相关,其中与睡眠质量有关的测量值(例如,睡眠效率)通常比单纯的睡眠时间受到更大的影响。效应大小通常较小:例如,4 种诊断中最大的幅度效应大小为β=-0.11(95%置信区间为-0.13 至-0.10,p=3×10-56,FDR=6×10-55),用于与终生住院的主要抑郁障碍诊断相关的睡眠效率。关联在各个血统和性别中基本一致,并且加速计衍生的测量值与自我报告的睡眠特征一致。局限性包括基于加速计的睡眠测量以及精神疾病诊断和加速计之间的时间滞后。
在这项研究中,我们观察到睡眠模式差异是具有终生精神疾病的个体的跨诊断特征,这表明无论诊断如何,都应考虑到这些差异。加速计为在精神科临床研究和实践中客观测量睡眠特性提供了一种可扩展的方法,即使在数万人中也是如此。