Students' Scientific Research Center, Tehran University of Medical Sciences, Tehran, Iran.
Department of Clinical Nutrition, School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences, Tehran, Iran.
BMJ. 2021 Oct 13;375:n2213. doi: 10.1136/bmj.n2213.
To examine the associations between dietary intake and tissue biomarkers of alpha linolenic acid (ALA) and risk of mortality from all causes, cardiovascular disease (CVD), and cancer.
Systematic review and meta-analysis of prospective cohort studies.
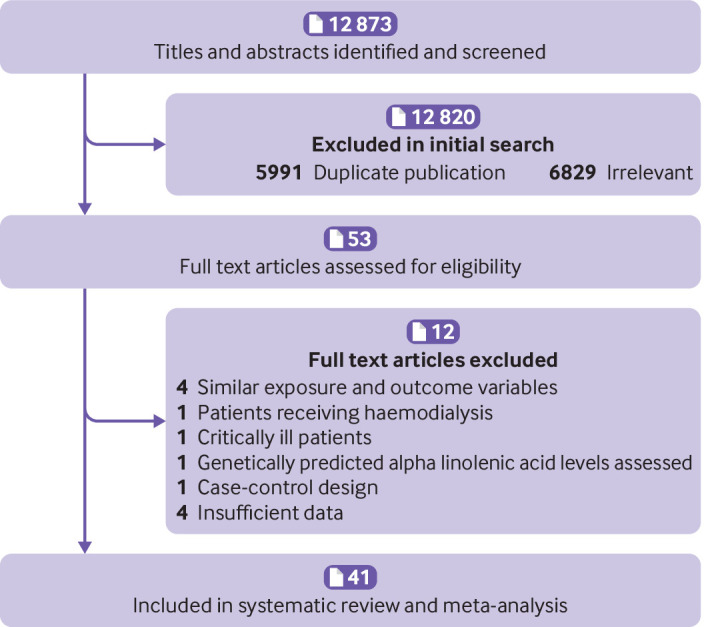
PubMed, Scopus, ISI Web of Science, and Google Scholar to 30 April 2021.
Prospective cohort studies that reported the risk estimates for death from all causes, CVD, and cancer.
Summary relative risks and 95% confidence intervals were calculated for the highest versus lowest categories of ALA intake using random effects and fixed effects models. Linear and non-linear dose-response analyses were conducted to assess the dose-response associations between ALA intake and mortality.
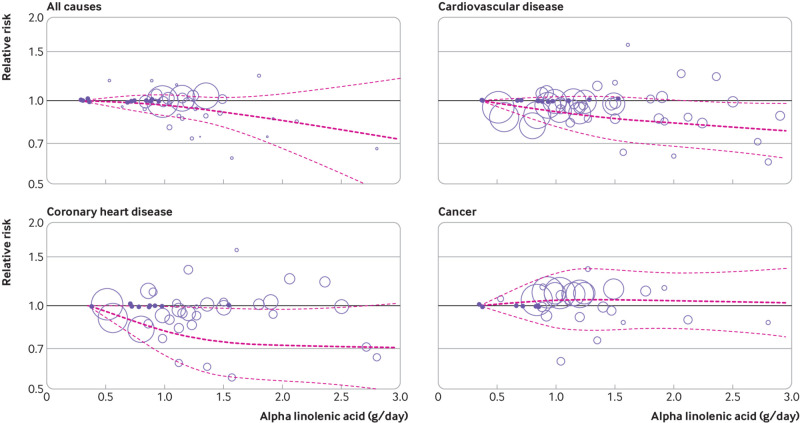
41 articles from prospective cohort studies were included in this systematic review and meta-analysis, totalling 1 197 564 participants. During follow-up ranging from two to 32 years, 198 113 deaths from all causes, 62 773 from CVD, and 65 954 from cancer were recorded. High intake of ALA compared with low intake was significantly associated with a lower risk of deaths from all causes (pooled relative risk 0.90, 95% confidence interval 0.83 to 0.97, I=77.8%, 15 studies), CVD (0.92, 0.86 to 0.99, I=48.2%, n=16), and coronary heart disease (CHD) (0.89, 0.81 to 0.97, I=5.6%, n=9), and a slightly higher risk of cancer mortality (1.06, 1.02 to 1.11, I=3.8%, n=10). In the dose-response analysis, a 1 g/day increase in ALA intake (equivalent to one tablespoon of canola oil or 0.5 ounces of walnut) was associated with a 5% lower risk of all cause (0.95, 0.91 to 0.99, I=76.2%, n=12) and CVD mortality (0.95, 0.91 to 0.98, I=30.7%, n=14). The pooled relative risks for the highest compared with lowest tissue levels of ALA indicated a significant inverse association with all cause mortality (0.95, 0.90 to 0.99, I=8.2%, n=26). Also, based on the dose-response analysis, each 1 standard deviation increment in blood concentrations of ALA was associated with a lower risk of CHD mortality (0.92, 0.86 to 0.98, I=37.1%, n=14).
The findings show that dietary ALA intake is associated with a reduced risk of mortality from all causes, CVD, and CHD, and a slightly higher risk of cancer mortality, whereas higher blood levels of ALA are associated with a reduced risk of all cause and CHD mortality only.
PROSPERO CRD42021229487.
探讨饮食中 α-亚麻酸(ALA)的摄入量与组织生物标志物与全因死亡率、心血管疾病(CVD)和癌症风险之间的关系。
对前瞻性队列研究进行系统评价和荟萃分析。
PubMed、Scopus、ISI Web of Science 和 Google Scholar 至 2021 年 4 月 30 日。
报告全因死亡、CVD 和癌症风险的最高与最低 ALA 摄入量的前瞻性队列研究。
使用随机效应和固定效应模型,计算 ALA 摄入量最高与最低组之间的总死亡率、CVD 死亡率和癌症死亡率的相对风险及 95%置信区间。进行线性和非线性剂量-反应分析,以评估 ALA 摄入量与死亡率之间的剂量-反应关系。
从前瞻性队列研究中纳入了 41 篇文章,共纳入 1197564 名参与者。在 2 至 32 年的随访期间,记录了 198113 例全因死亡、62773 例 CVD 死亡和 65954 例癌症死亡。与低摄入量相比,ALA 高摄入量与全因死亡率(合并相对风险 0.90,95%置信区间 0.83 至 0.97,I=77.8%,15 项研究)、CVD 死亡率(0.92,0.86 至 0.99,I=48.2%,n=16)和冠心病(CHD)死亡率(0.89,0.81 至 0.97,I=5.6%,n=9)显著降低相关,而癌症死亡率则略有升高(1.06,1.02 至 1.11,I=3.8%,n=10)。在剂量-反应分析中,ALA 摄入量增加 1 克/天(相当于一汤匙菜籽油或 0.5 盎司核桃)与全因死亡率(0.95,0.91 至 0.99,I=76.2%,n=12)和 CVD 死亡率(0.95,0.91 至 0.98,I=30.7%,n=14)降低 5%相关。ALA 组织水平最高与最低水平之间的汇总相对风险表明与全因死亡率呈显著负相关(0.95,0.90 至 0.99,I=8.2%,n=26)。此外,基于剂量-反应分析,血液中 ALA 浓度每增加 1 个标准差,与 CHD 死亡率降低相关(0.92,0.86 至 0.98,I=37.1%,n=14)。
研究结果表明,饮食中 ALA 的摄入量与全因死亡率、CVD 和 CHD 风险降低有关,而癌症死亡率则略有升高,而血液中 ALA 水平升高仅与全因和 CHD 死亡率降低有关。
PROSPERO CRD42021229487。