Tousidonis Manuel, Ochandiano Santiago, Navarro-Cuellar Carlos, Navarro-Vila Carlos, López de Atalaya Javier, Maza Cristina, Lopez Lopez Ana María, Navarro-Cuellar Ignacio, García Sevilla Alba, Arenas de Frutos Gema, Antunez-Conde Raul, Planells Del Pozo Paloma, Salmeron Jose Ignacio
Department of Oral and Maxillofacial Surgery, Hospital General Universitario Gregorio Marañón, 28007 Madrid, Spain.
Instituto de Investigación Sanitaria Gregorio Marañón (IISGM), 28007 Madrid, Spain.
J Clin Med. 2025 Aug 1;14(15):5435. doi: 10.3390/jcm14155435.
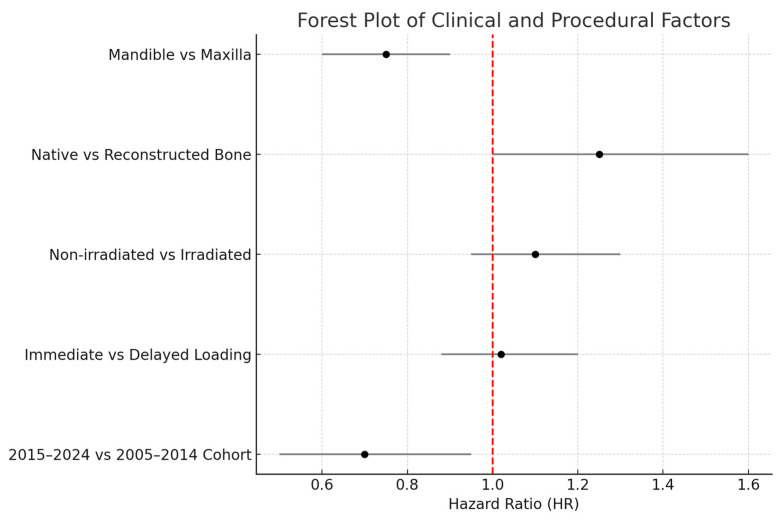
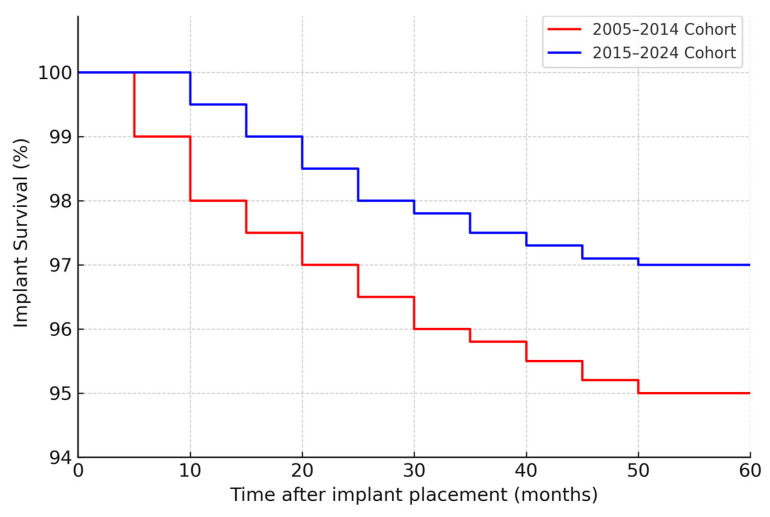
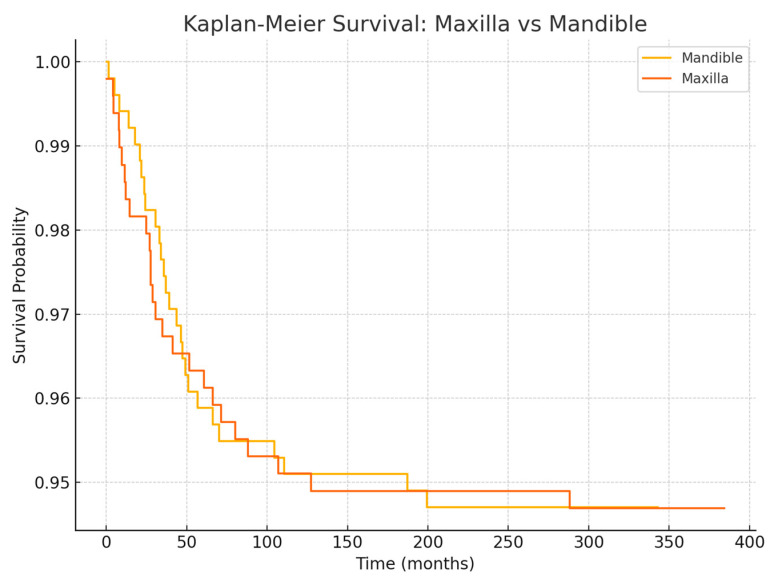
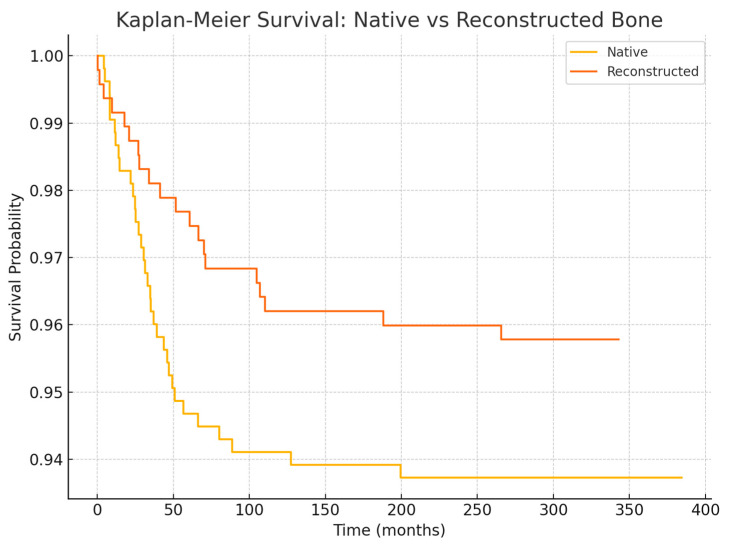
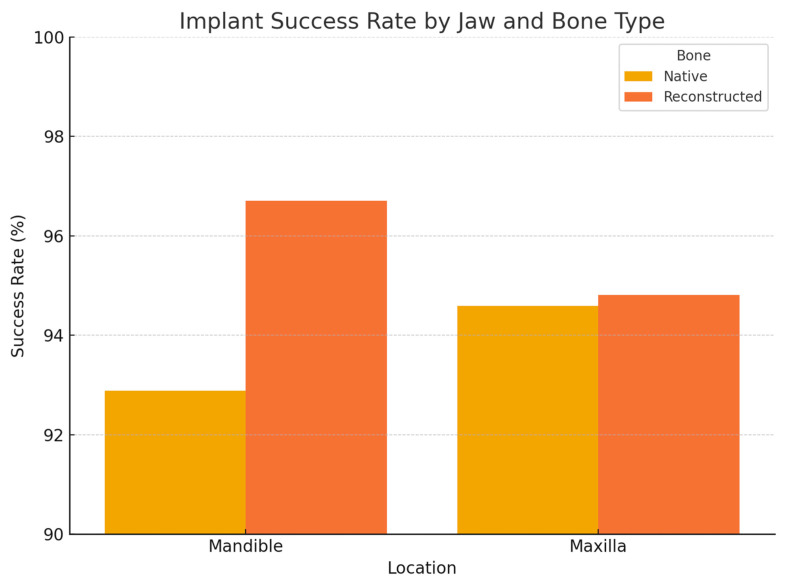
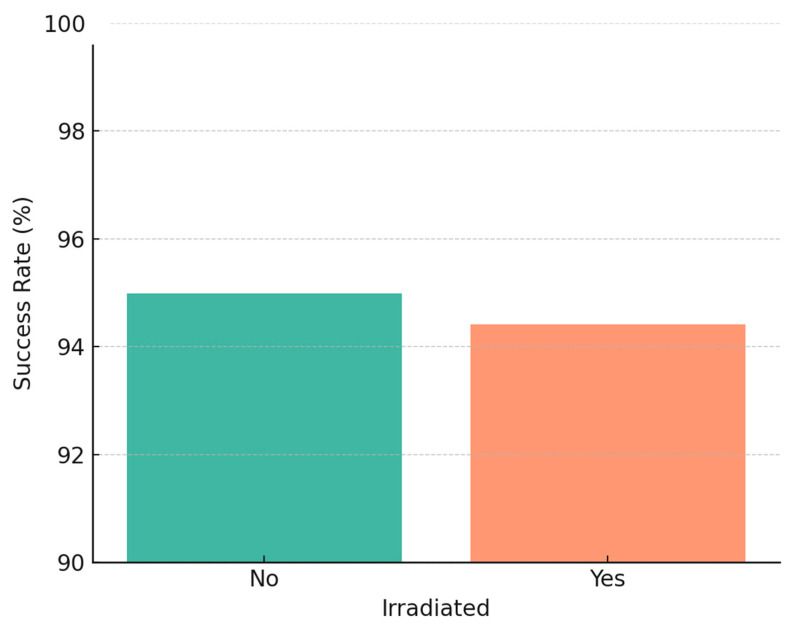
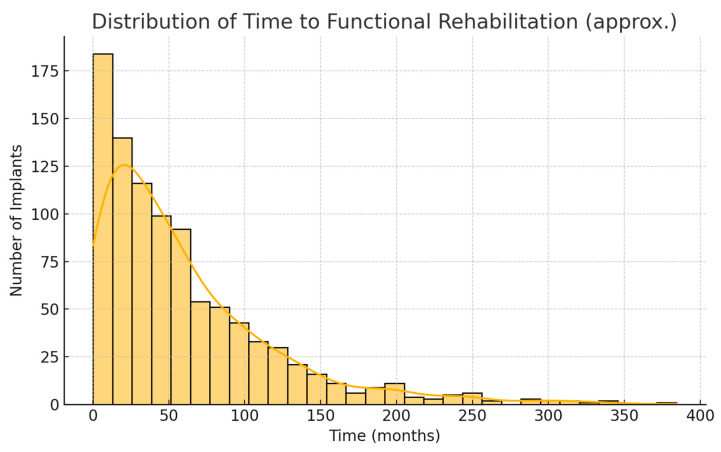
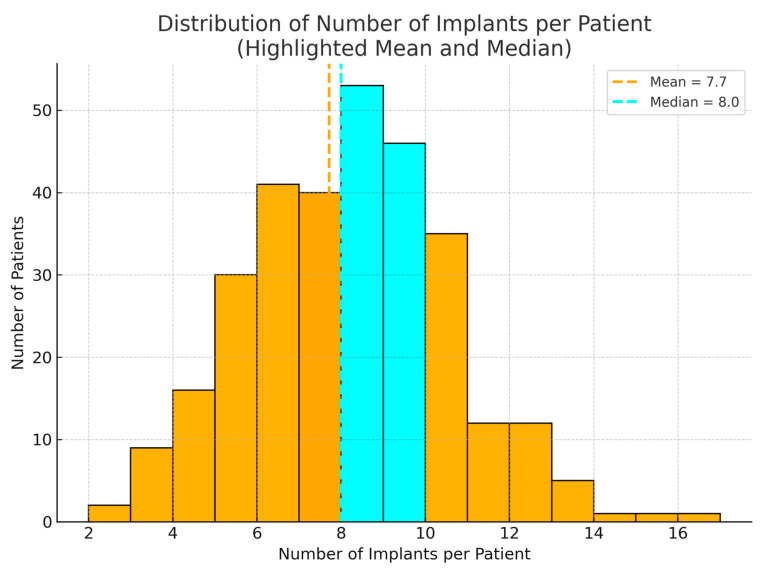
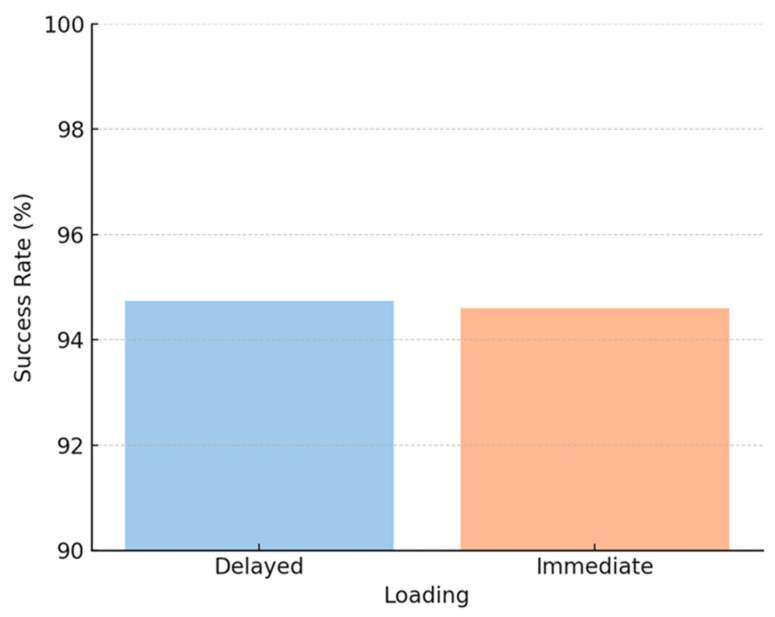
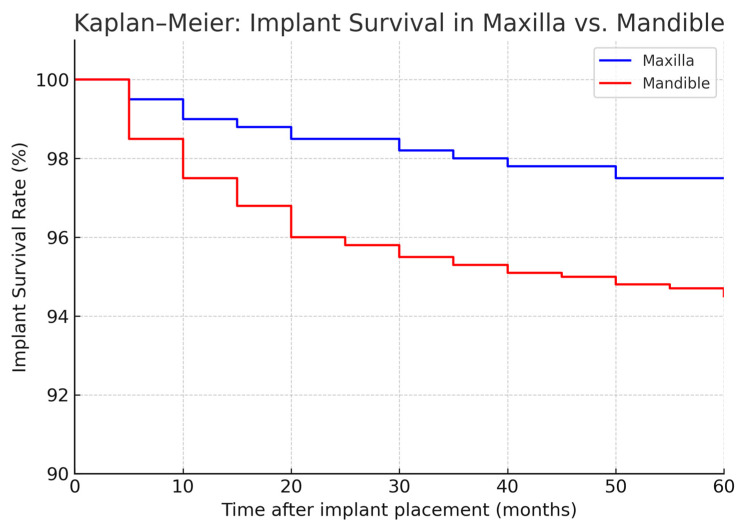
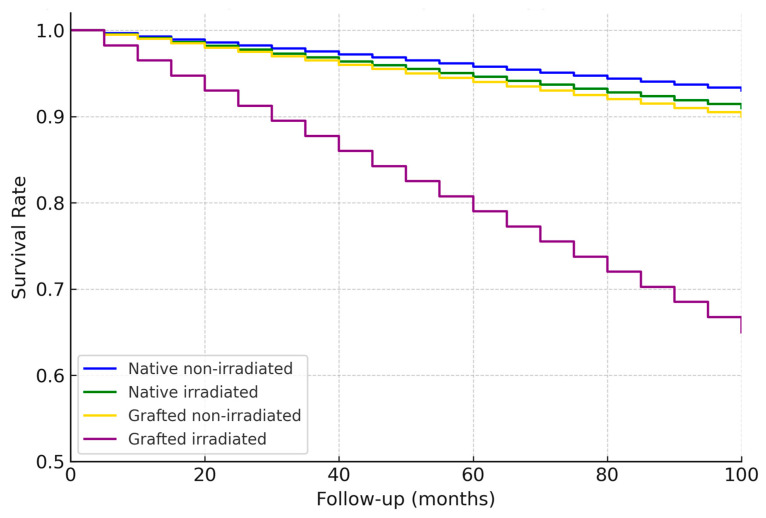
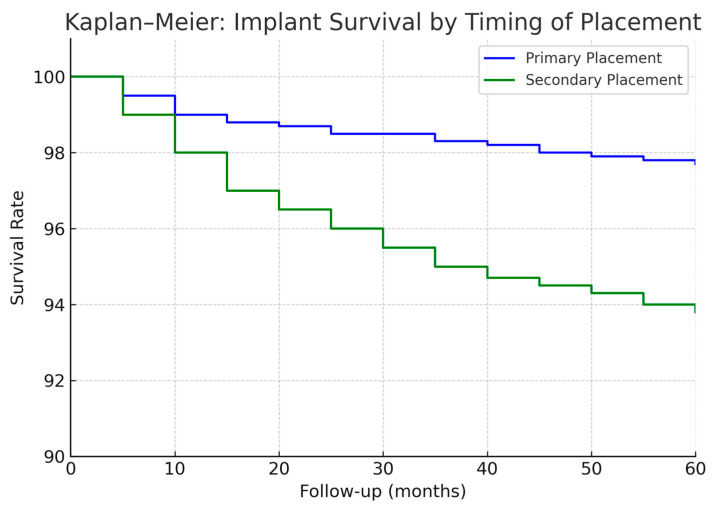
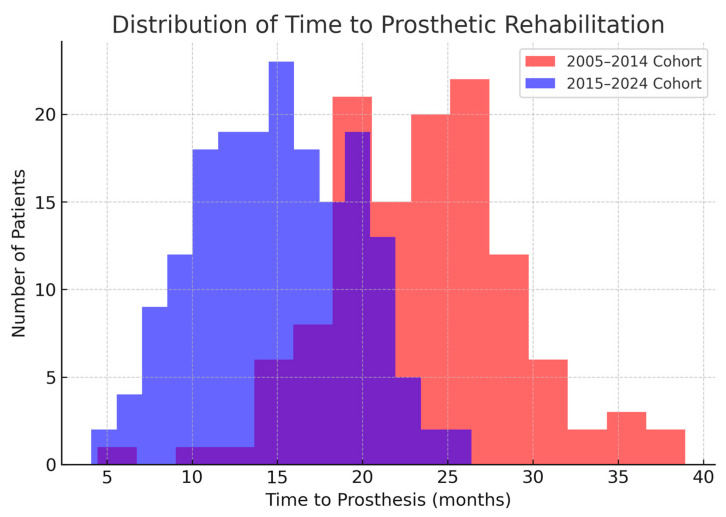
Oral cancer resection often leads to maxillofacial defects and dentition loss, compromising patients' quality of life. Implant-supported prosthetic rehabilitation offers a reliable solution to restore function, though factors such as bone reconstruction, radiotherapy, and timing of implant placement (immediate vs. delayed) may influence outcomes. This study aimed to evaluate long-term implant survival and rehabilitation timelines in oncologic patients, comparing two cohorts (2005-2014 and 2015-2024) to assess the impact of evolving clinical practices. A retrospective cohort study was conducted at Hospital General Universitario Gregorio Marañón (Madrid, Spain), including 304 patients who underwent ablative oral cancer surgery and subsequent implant-based rehabilitation between 2005 and 2024. Data on demographics, oncologic treatment, reconstruction, implant timing, and prosthetic rehabilitation were collected. Outcomes were compared using Kaplan-Meier analysis and appropriate statistical tests between the 2005-2014 ( = 122) and 2015-2024 ( = 182) cohorts. A total of 2341 Ticare Implants were placed, supporting 281 prostheses. Implant placement during primary surgery increased from 41% to 71% ( < 0.001). The median time from surgery to prosthesis significantly decreased from 24 to 15 months ( < 0.001). Five-year implant survival was 95% in the early cohort versus 97% in the later cohort. Implant survival was comparable between irradiated and non-irradiated patients (~94-96%). Fixed prostheses became more frequent (92% vs. 79%, = 0.002). Implant-supported rehabilitation in oncologic patients is highly feasible and durable, with improved timelines and functional outcomes associated with early implant placement and modern digital planning strategies.
口腔癌切除术后常导致颌面缺损和牙列缺失,影响患者生活质量。种植体支持的修复性康复为恢复功能提供了可靠的解决方案,不过诸如骨重建、放疗以及种植体植入时机(即刻植入与延迟植入)等因素可能会影响治疗效果。本研究旨在评估肿瘤患者种植体的长期存留率及康复时间线,比较两个队列(2005 - 2014年和2015 - 2024年)以评估临床实践演变的影响。在西班牙马德里格雷戈里奥·马拉尼翁大学综合医院进行了一项回顾性队列研究,纳入了2005年至2024年间接受口腔癌切除手术及后续种植体支持康复治疗的304例患者。收集了人口统计学、肿瘤治疗、重建、种植体植入时机及修复性康复等方面的数据。采用Kaplan - Meier分析及适当的统计学检验对2005 - 2014年队列(n = 122)和2015 - 2024年队列(n = 182)的结果进行比较。共植入2341枚Ticare种植体,支持281个修复体。一期手术时种植体植入率从41%增至71%(P < 0.001)。从手术到佩戴修复体的中位时间从24个月显著降至15个月(P < 0.001)。早期队列的种植体5年存留率为95%,后期队列为97%。放疗患者与未放疗患者的种植体存留率相当(约94% - 96%)。固定修复体更为常见(92%对79%,P = 0.002)。肿瘤患者种植体支持的康复治疗高度可行且持久,早期种植体植入及现代数字化规划策略可改善治疗时间线和功能结局。