Department of Clinical Tropical Medicine, Faculty of Tropical Medicine, Mahidol University, Bangkok, 10400, Thailand.
Medical Technology, School of Allied Health Sciences, Walailak University, Tha Sala, Nakhon Si Thammarat, 80160, Thailand.
Parasit Vectors. 2021 Oct 23;14(1):545. doi: 10.1186/s13071-021-05045-1.
Malaria and visceral leishmaniasis (VL) co-infection can occur due to the overlapping geographical distributions of these diseases; however, only limited data of this co-infection have been reported and reviewed. This study aimed to explore the pooled prevalence and characteristics of this co-infection using a systematic review approach.
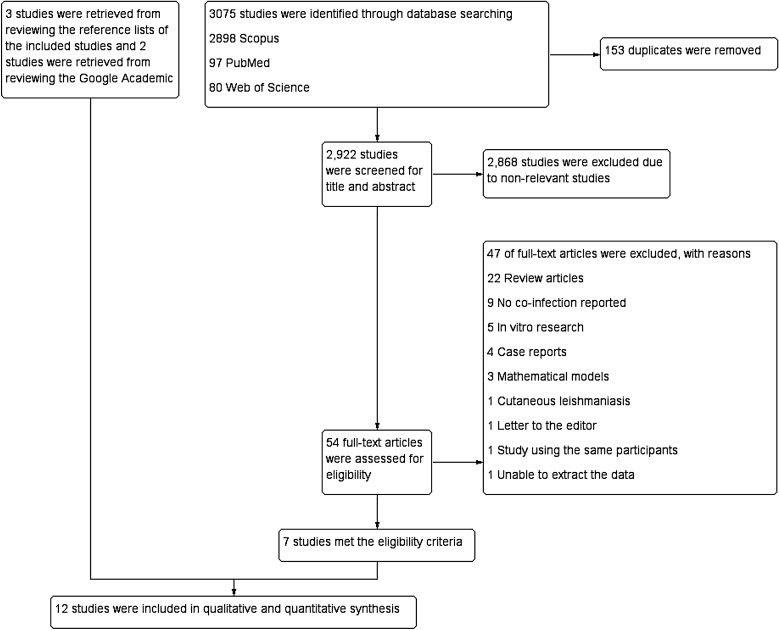
The PubMed, Web of Science and Scopus databases were searched for relevant studies. The quality of these studies was assessed in accordance with strengthening the reporting of observational studies in epidemiology (STROBE) guidelines. The numbers of individuals co-infected with Plasmodium and VL and the total numbers of individuals with VL were used to estimate the pooled prevalence using random-effects models. Differences in age, sex and the presence of anemia and malnutrition on admission were compared between co-infected individuals and individuals with VL using a random-effects model; the results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Heterogeneity among the included studies was assessed and quantified using Cochrane Q and I statistics.
Of the 3075 studies identified, 12 met the eligibility criteria and were included in this systematic review. The pooled prevalence of Plasmodium infection among the 6453 individuals with VL was 13%, with substantial heterogeneity of the data (95% CI 7-18%, I 97.9%). Subgroup analysis demonstrated that the highest prevalence of co-infection occurred in African countries, whereas the lowest prevalence occurred in Asian countries. Patients aged < 5 years had higher odds of having co-infection than having VL (co-infection, n = 202; VL, n = 410) (OR 1.66, 95% CI 1.37-2.01, I 0%; P < 0.0001), whereas patients aged 20-29 years had lower odds of having co-infection than having VL (co-infection, n = 170; VL, n = 699) (OR 0.75, 95% CI 0.60-0.93, I 18%; P = 0.01). Male patients had equivalent odds of having co-infection and having VL (co-infection, n = 525; VL, n = 2232) (OR 0.92, 95% CI 0.078-1.08, I 0%; P = 0.29). Patients with co-infection had lower odds of having anemia at admission than those with VL (co-infection, n = 902; VL, n = 2939) (OR 0.64, 95% CI 0.44-0.93, I 0%; P = 0.02). No difference in malnutrition at admission was found in the meta-analysis.
The prevalence of malaria co-infection among individuals with VL was heterogeneous and ranged from 7 to 18%, depending on geographical area. Age and anemia at admission were associated with co-infection status. Further longitudinal studies are needed to determine if co-infection with malaria has an impact on the severity of VL.
疟疾和内脏利什曼病(VL)可能因这两种疾病的地理分布重叠而发生合并感染;然而,仅有有限的此类合并感染的数据被报道和综述。本研究旨在通过系统综述方法来探讨这种合并感染的合并患病率和特征。
在 PubMed、Web of Science 和 Scopus 数据库中检索相关研究。根据加强观察性研究报告的流行病学(STROBE)指南评估这些研究的质量。使用随机效应模型,根据合并感染疟原虫和 VL 的个体数量和 VL 个体的总数,估算合并感染的合并患病率。使用随机效应模型比较合并感染个体和 VL 个体入院时的年龄、性别和贫血及营养不良的差异;结果表示为比值比(OR)和 95%置信区间(CI)。使用 Cochrane Q 和 I 统计量评估纳入研究的异质性并进行量化。
在 3075 项研究中,有 12 项符合纳入标准并被纳入本系统综述。在 6453 例 VL 个体中,疟原虫感染的合并患病率为 13%,数据存在显著异质性(95%CI 7-18%,I 97.9%)。亚组分析表明,合并感染的最高患病率出现在非洲国家,而在亚洲国家则最低。年龄<5 岁的患者比患有 VL 的患者更有可能合并感染(合并感染,n=202;VL,n=410)(OR 1.66,95%CI 1.37-2.01,I 0%;P<0.0001),而年龄 20-29 岁的患者比患有 VL 的患者更不可能合并感染(合并感染,n=170;VL,n=699)(OR 0.75,95%CI 0.60-0.93,I 18%;P=0.01)。男性患者与患有 VL 的患者合并感染的可能性相同(合并感染,n=525;VL,n=2232)(OR 0.92,95%CI 0.078-1.08,I 0%;P=0.29)。合并感染的患者入院时贫血的可能性比患有 VL 的患者低(合并感染,n=902;VL,n=2939)(OR 0.64,95%CI 0.44-0.93,I 0%;P=0.02)。在荟萃分析中未发现入院时营养不良的差异。
VL 患者中疟疾合并感染的患病率存在异质性,范围为 7-18%,具体取决于地理区域。年龄和入院时的贫血与合并感染状况相关。需要进一步的纵向研究来确定疟疾合并感染是否会影响 VL 的严重程度。