Section of Epidemiology and Biostatistics, Faculty of Medical and Health Sciences, The University of Auckland, Auckland Mail Centre, Private Bag 92019, Auckland, 1142, New Zealand.
Department of General Practice and Primary Health Care, Faculty of Medical and Health Sciences, The University of Auckland, Auckland Mail Centre, Private Bag 92019, Auckland, 1142, New Zealand.
BMC Cardiovasc Disord. 2021 Oct 24;21(1):515. doi: 10.1186/s12872-021-02313-x.
Pacific people experience a disproportionate burden of cardiovascular disease (CVD), whether they remain in their country of origin or migrate to higher-income countries, such as Australia, Aotearoa New Zealand or the United States of America. We sought to determine whether the CVD health needs of Pacific people vary according to their ethnicity or place of birth.
We conducted a systematic review of medical research databases and grey literature to identify relevant data published up to 2020. Texts were included if they contained original data stratified by Pacific-specific ethnicity or place of birth on the burden or management of CVD, and were assessed as having good quality using a National Heart, Lung, and Blood Institute quality assessment tool. The protocol for this review was registered with the Open Science Forum ( https://doi.org/10.17605/OSF.IO/X7NR6 ).
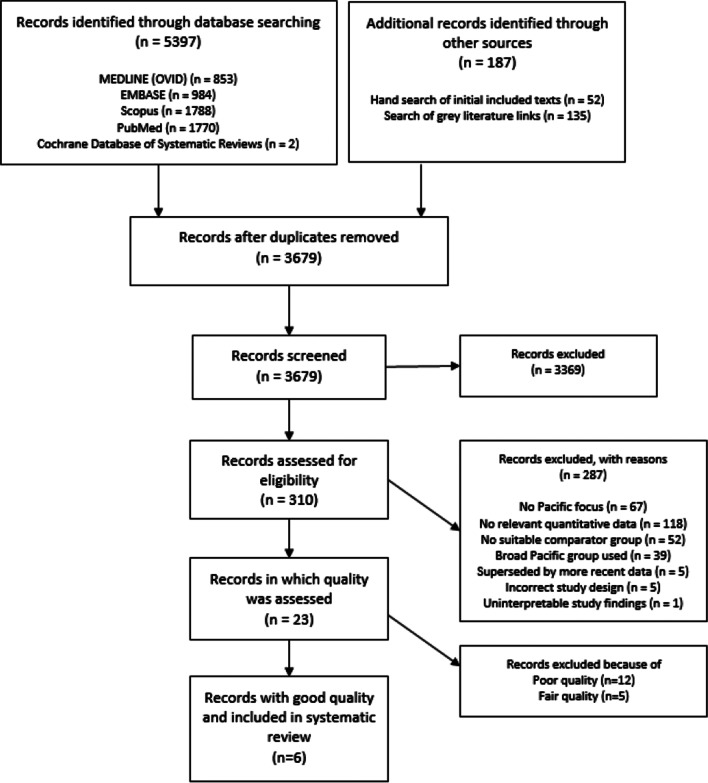
Of 3679 texts identified, 310 full texts were reviewed and the quality of 23 of these assessed, using the pre-defined search strategy. Six items (four reports, one article, one webpage) of good quality met the review eligibility criteria. All included texts provided data on epidemiology but only one reported on the management of CVD. Four texts were of Pacific populations in Pacific Island countries and two were of Pacific diaspora in other countries. Data from the Global Burden of Disease study, which provided estimates for the greatest number of Pacific countries, showed substantial differences in mortality rates between Pacific countries for every CVD type. For example, the mortality rate per 100,000 for ischemic heart disease (IHD) ranged from 103.41 in the Cook Islands to 430.35 in the Solomon Islands. A New Zealand-based report showed differences in CVD rates by Pacific ethnicity (e.g. the age-standardised prevalence of IHD per 1,000 population in Auckland ranged from 107.8 (Niuean) to 138 among Cook Islands Māori (p < 0.001)).
This review of published studies reveals that the epidemiology of CVD among Pacific people varies by specific ethnic groups, place of birth, and country of residence. There is a critical need for high-quality contemporary ethnic-specific Pacific data to respond to the diverse CVD health needs in these underrepresented groups.
太平洋人民无论在原籍国还是移民到澳大利亚、新西兰或美国等高收入国家,都面临不成比例的心血管疾病(CVD)负担。我们试图确定太平洋人民的 CVD 健康需求是否因种族或出生地而异。
我们对医学研究数据库和灰色文献进行了系统回顾,以确定截至 2020 年发表的相关数据。如果文本包含按太平洋特定种族或出生地划分的 CVD 负担或管理的原始数据,并且使用国家心脏、肺和血液研究所质量评估工具评估为高质量,则将其纳入。该综述的方案在开放科学论坛(https://doi.org/10.17605/OSF.IO/X7NR6 )上进行了注册。
在 3679 篇文章中,有 310 篇全文进行了审查,使用预先定义的搜索策略评估了其中 23 篇的质量。6 项(4 份报告、1 篇文章、1 个网页)高质量的项目符合审查标准。所有纳入的文章都提供了流行病学数据,但只有一篇报告了 CVD 的管理。有 4 篇文章是关于太平洋岛国的太平洋人群,有 2 篇文章是关于其他国家的太平洋侨民。全球疾病负担研究的数据为大多数太平洋国家提供了估计数,显示出每种 CVD 类型在太平洋国家之间死亡率的巨大差异。例如,每 10 万人的缺血性心脏病(IHD)死亡率在库克群岛为 103.41,在所罗门群岛为 430.35。一份新西兰的报告显示了太平洋族裔之间 CVD 率的差异(例如,奥克兰每 1000 人口的 IHD 标准化流行率,从纽埃人 107.8 到毛利人库克群岛 138 不等(p<0.001))。
对已发表研究的综述表明,太平洋人民的 CVD 流行病学因特定族裔、出生地和居住国而异。迫切需要高质量的当代特定族裔太平洋数据来满足这些代表性不足群体多样化的 CVD 健康需求。