Division of Cardiology, Massachusetts General Hospital, Boston, Massachusetts, USA.
Cardiovascular Performance Program, Massachusetts General Hospital, Boston, Massachusetts, USA.
Br J Sports Med. 2022 Aug;56(16):913-918. doi: 10.1136/bjsports-2021-104644. Epub 2021 Nov 1.
To assess the prevalence and clinical implications of persistent or exertional cardiopulmonary symptoms in young competitive athletes following SARS-CoV-2 infection.
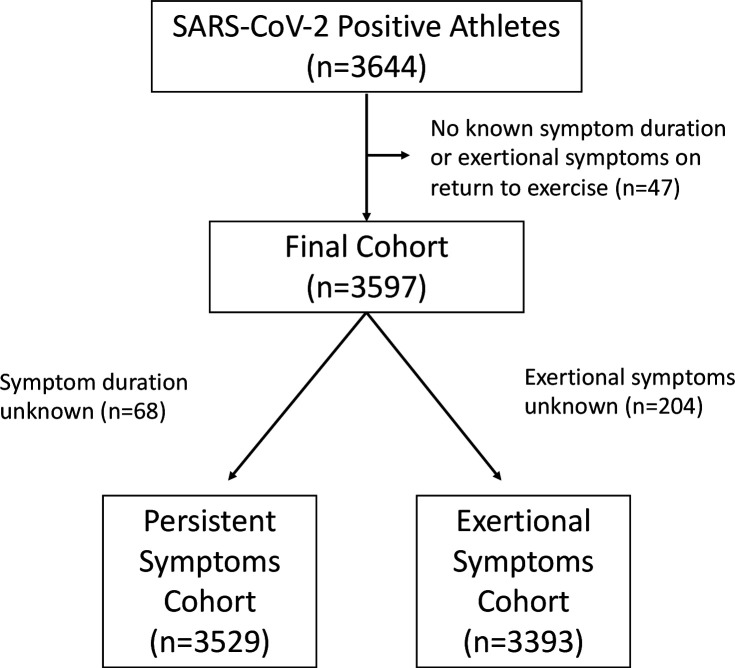
This observational cohort study from the Outcomes Registry for Cardiac Conditions in Athletes included 3597 US collegiate athletes after SARS-CoV-2 infection. Clinical characteristics, advanced diagnostic testing and SARS-CoV-2-associated sequelae were compared between athletes with persistent symptoms >3 weeks, exertional symptoms on return to exercise and those without persistent or exertional symptoms.
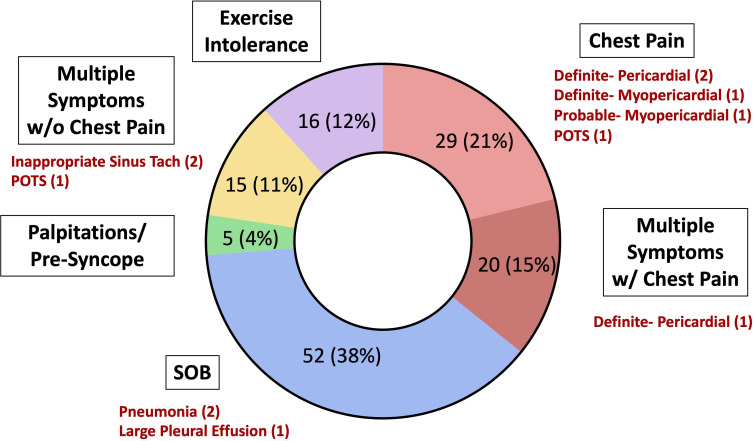
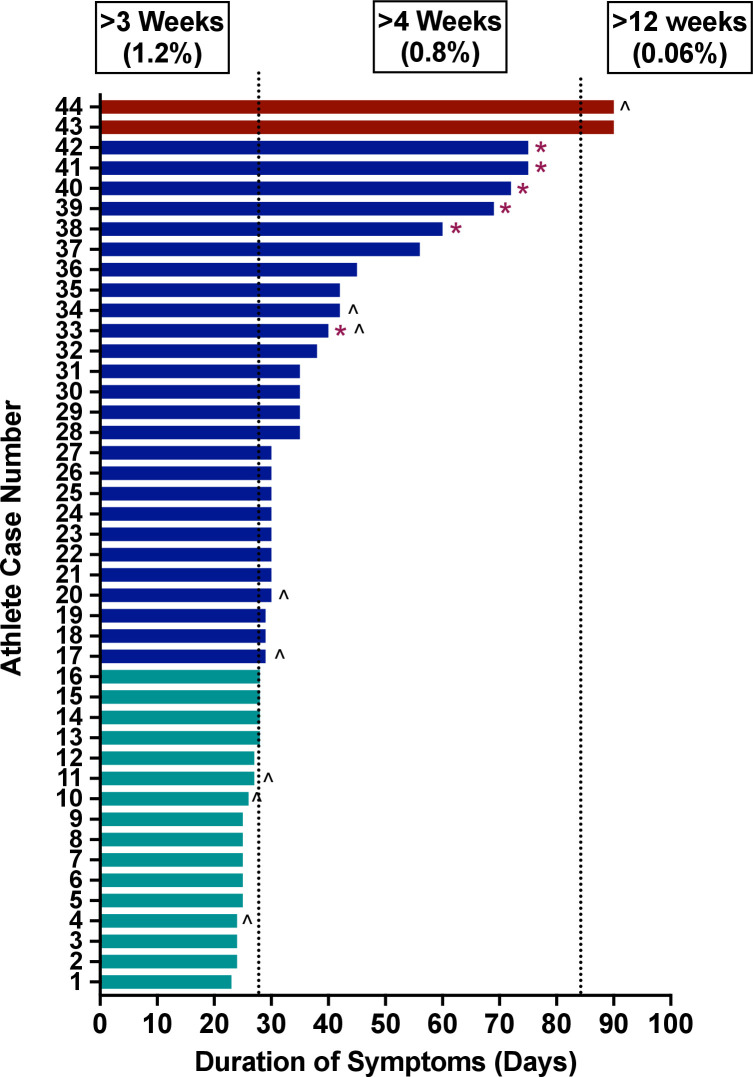
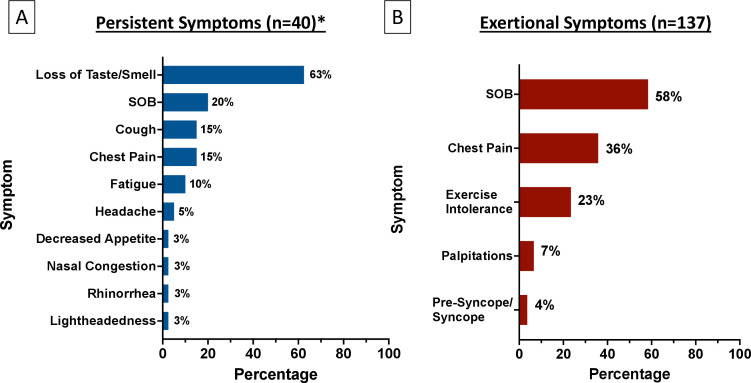
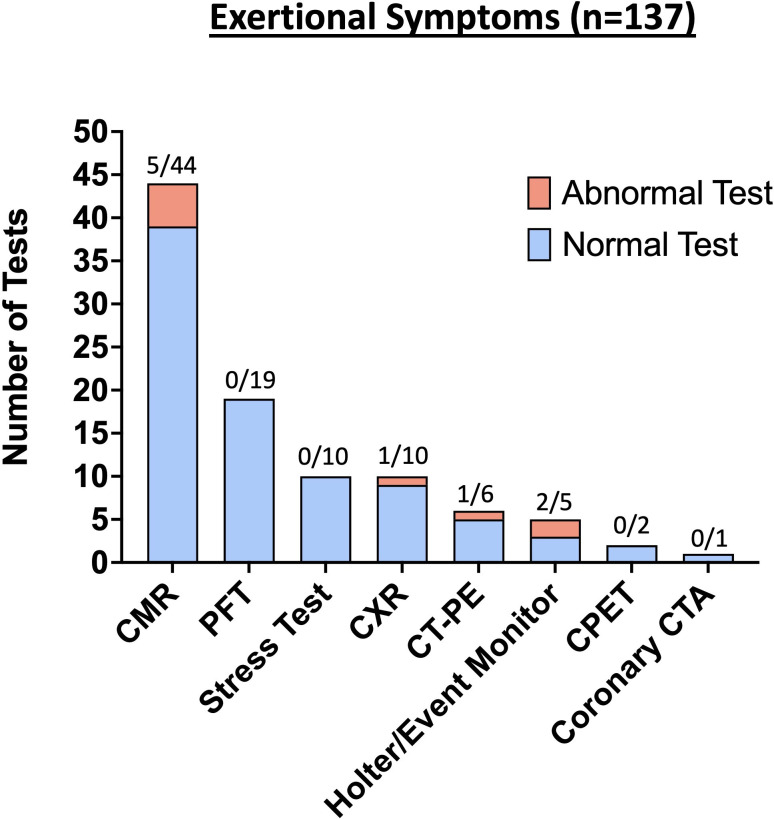
Among 3597 athletes (mean age 20 years (SD, 1 year), 34% female), data on persistent and exertional symptoms were reported in 3529 and 3393 athletes, respectively. Persistent symptoms >3 weeks were present in 44/3529 (1.2%) athletes with 2/3529 (0.06%) reporting symptoms >12 weeks. Exertional cardiopulmonary symptoms were present in 137/3393 (4.0%) athletes. Clinical evaluation and diagnostic testing led to the diagnosis of SARS-CoV-2-associated sequelae in 12/137 (8.8%) athletes with exertional symptoms (five cardiac involvement, two pneumonia, two inappropriate sinus tachycardia, two postural orthostatic tachycardia syndrome and one pleural effusion). No SARS-CoV-2-associated sequelae were identified in athletes with isolated persistent symptoms. Of athletes with chest pain on return to exercise who underwent cardiac MRI (CMR), 5/24 (20.8%) had probable or definite cardiac involvement. In contrast, no athlete with exertional symptoms without chest pain who underwent CMR (0/20) was diagnosed with probable or definite SARS-CoV-2 cardiac involvement.
Collegiate athletes with SARS-CoV-2 infection have a low prevalence of persistent or exertional symptoms on return to exercise. Exertional cardiopulmonary symptoms, specifically chest pain, warrant a comprehensive evaluation.
评估 SARS-CoV-2 感染后年轻竞技运动员持续或运动后心肺症状的流行情况及其临床意义。
这项来自运动员心脏疾病结果注册库的观察性队列研究纳入了 3597 名美国大学生运动员,这些运动员曾感染 SARS-CoV-2。比较了持续症状>3 周、运动后出现症状和无持续或运动后症状的运动员之间的临床特征、高级诊断检测和 SARS-CoV-2 相关后遗症。
在 3597 名运动员(平均年龄 20 岁[标准差,1 岁],34%为女性)中,分别有 3529 名和 3393 名运动员报告了持续和运动后症状数据。3529 名运动员中有 44 名(1.2%)持续症状>3 周,其中 2 名(0.06%)报告症状>12 周。3393 名运动员中有 137 名(4.0%)出现运动后心肺症状。137 名有运动后症状的运动员中,有 12 名(8.8%)通过临床评估和诊断性检测诊断为 SARS-CoV-2 相关后遗症,包括 5 例心脏受累、2 例肺炎、2 例不适当窦性心动过速、2 例体位性心动过速综合征和 1 例胸腔积液。孤立性持续症状的运动员未发现 SARS-CoV-2 相关后遗症。在因运动后胸痛而接受心脏 MRI(CMR)的运动员中,5/24(20.8%)有明确或可能的心脏受累。相比之下,20 名无胸痛的运动后有症状的运动员中无一例(0/20)经 CMR 诊断为 SARS-CoV-2 心脏受累的可能性或明确性。
感染 SARS-CoV-2 的大学生运动员在恢复运动后持续或运动后出现症状的发生率较低。运动后心肺症状,特别是胸痛,需要全面评估。