Department of Ophthalmology, Peking University People's Hospital; College of Optometry, Beijing, China.
University Health Science Center; Beijing Key Laboratory of Diagnosis and Therapy of Retinal and Choroid Diseases, Beijing, China.
Invest Ophthalmol Vis Sci. 2021 Nov 1;62(14):6. doi: 10.1167/iovs.62.14.6.
To investigate the biometric differences of anterior segment parameters between fellow eyes of acute primary angle closure (F-APAC) and chronic primary angle closure glaucoma (F-CPACG) to get information about differences between APAC and CPAC.
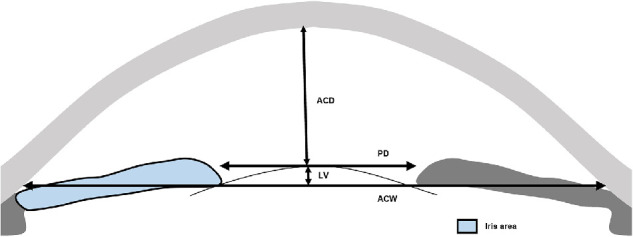
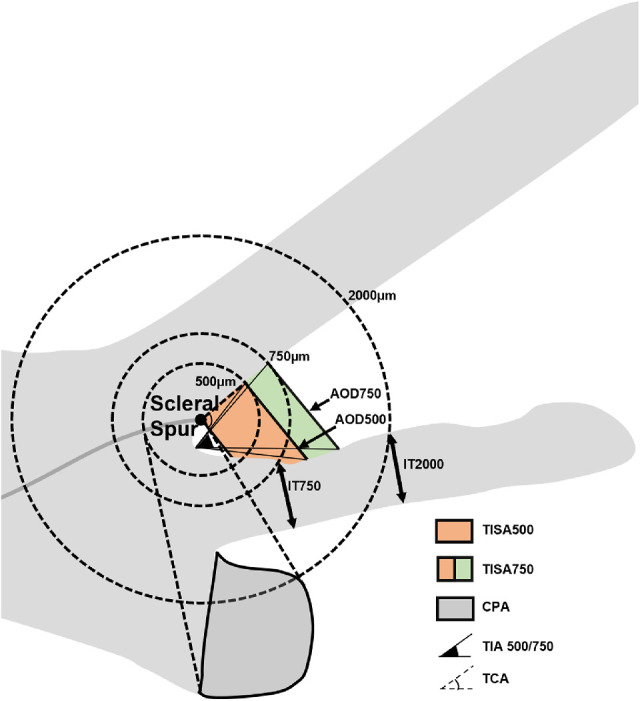
Patients with F-APAC and F-CPACG without prior treatment were enrolled from glaucoma clinics. Parameters were measured on ultrasound biomicroscopy images, including pupil diameter, lens vault (LV), anterior chamber depth, anterior chamber width, iris area, iris thickness (IT 750 and 2000), angle-opening distance (AOD 500 and 750), trabecular-iris space area (TISA 500 and 750), trabecular iris angle (TIA 500 and 750), trabecular-ciliary angle, and ciliary process area. Multivariate logistic regression analysis was performed to determine the most important parameters associated with F-APAC compared with F-CPACG.
Fifty-five patients with APAC and 55 patients with CPACG were examined. The anterior chamber depth, IT 750, AOD 750, trabecular iris angle 750, and trabecular-ciliary angle were smaller, and LV and ciliary process area were greater in F-APAC as compared with F-CPACG (P ≤ 0.01). Multivariate logistic regression showed that thinner IT 750, smaller AOD 750, and larger LV were significantly associated with F-APAC (P < 0.01). IT 750 (area under the curve, 0.703) performed relatively better than AOD 750 (area under the curve, 0.696) in distinguishing F-APAC from F-CPACG, with the best cutoff of 0.404 mm and 0.126 mm, respectively.
Compared with F-CPACG, F-APAC had thinner peripheral iris, narrower anterior chamber angle, shallower anterior chamber depth, greater LV, larger and anteriorly positioned ciliary body. IT 750, AOD 750, and LV played important roles in distinguishing eyes predisposed to APAC or CPAC.
研究急性原发性闭角型青光眼(F-APAC)和慢性原发性闭角型青光眼(F-CPACG)对眼前节参数的生物测量差异,以了解 APAC 和 CPAC 之间的差异。
从青光眼诊所招募未经治疗的 F-APAC 和 F-CPACG 患者。使用超声生物显微镜图像测量瞳孔直径、晶状体拱高(LV)、前房深度、前房宽度、虹膜面积、虹膜厚度(IT750 和 2000)、房角开放距离(AOD500 和 750)、小梁虹膜空间面积(TISA500 和 750)、小梁虹膜角度(TIA500 和 750)、小梁睫状体角和睫状体突面积。采用多变量逻辑回归分析确定与 F-CPACG 相比,与 F-APAC 最相关的最重要参数。
共检查了 55 例 APAC 患者和 55 例 CPACG 患者。与 F-CPACG 相比,F-APAC 的前房深度、IT750、AOD750、小梁虹膜角度 750 和小梁睫状体角较小,LV 和睫状体突面积较大(P≤0.01)。多变量逻辑回归显示,较薄的 IT750、较小的 AOD750 和较大的 LV 与 F-APAC 显著相关(P<0.01)。IT750(曲线下面积,0.703)在区分 F-APAC 与 F-CPACG 方面优于 AOD750(曲线下面积,0.696),最佳截断值分别为 0.404mm 和 0.126mm。
与 F-CPACG 相比,F-APAC 的周边虹膜较薄,前房角较窄,前房深度较浅,LV 较大,睫状体更靠前。IT750、AOD750 和 LV 在区分易发生 APAC 或 CPAC 的眼睛方面发挥重要作用。