Departments of Anesthesiology, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts.
the Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts.
Anesthesiology. 2021 Dec 1;135(6):1132-1152. doi: 10.1097/ALN.0000000000004046.
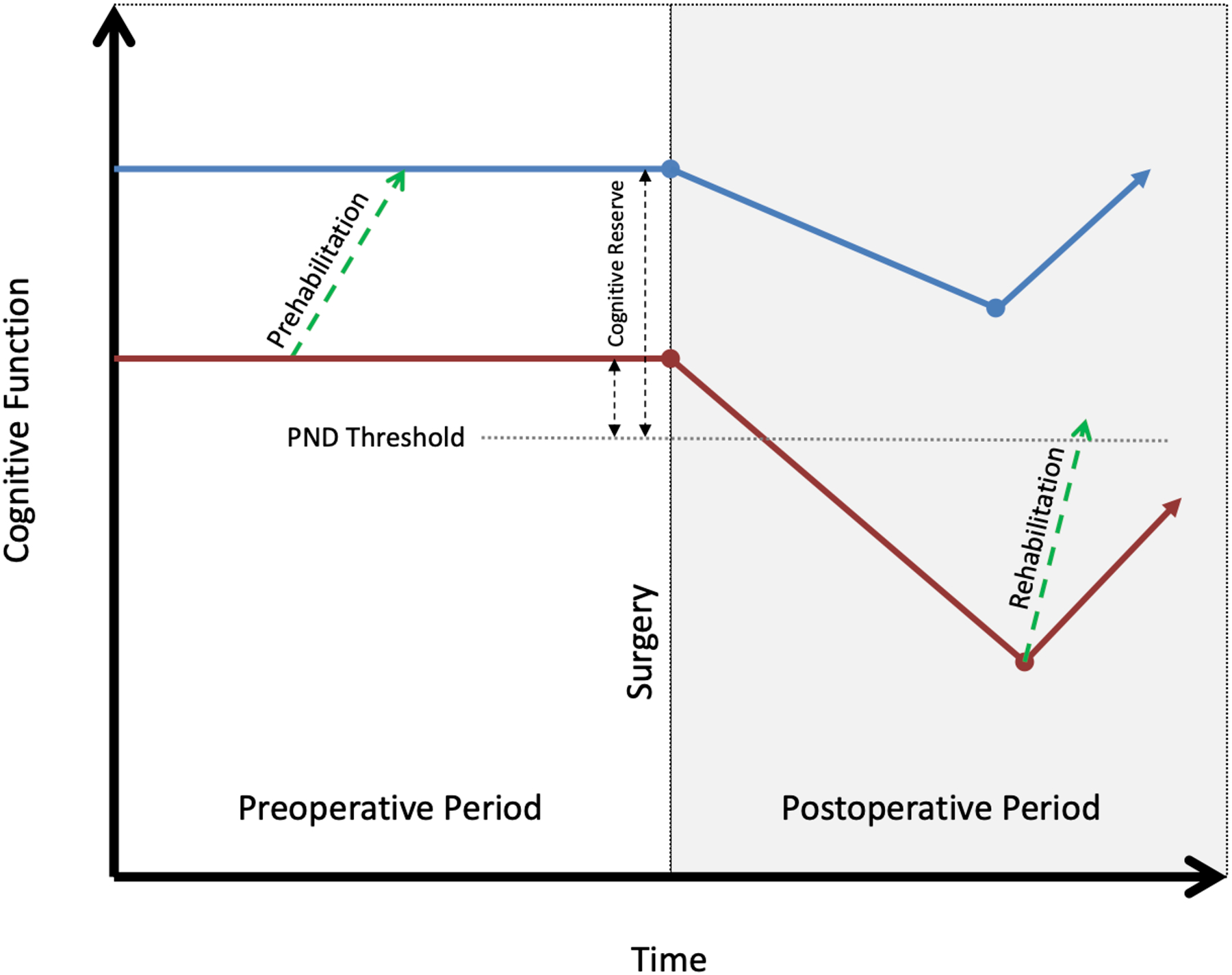
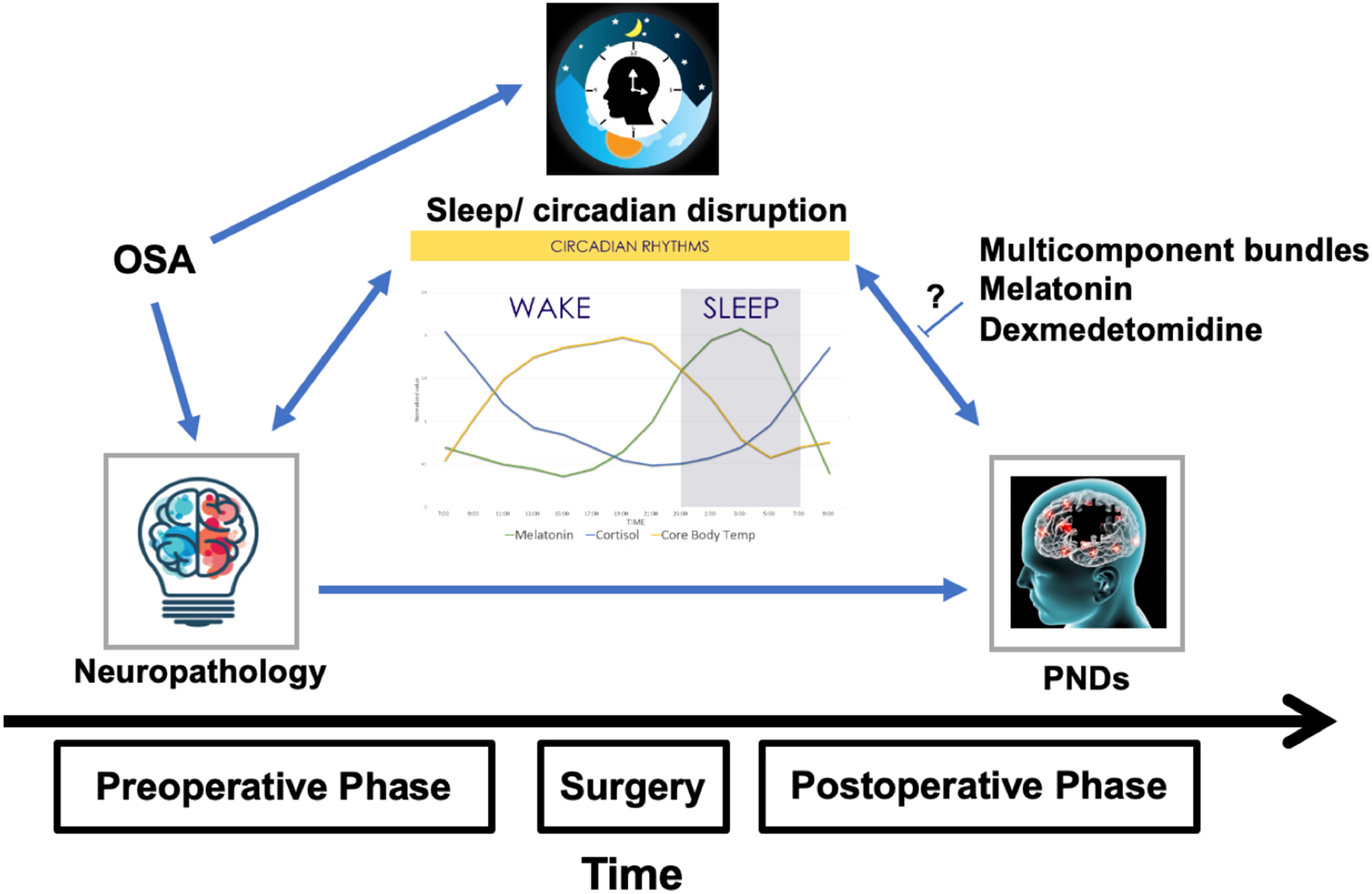
The prevention of perioperative neurocognitive disorders is a priority for patients, families, clinicians, and researchers. Given the multiple risk factors present throughout the perioperative period, a multicomponent preventative approach may be most effective. The objectives of this narrative review are to highlight the importance of sleep, pain, and cognition on the risk of perioperative neurocognitive disorders and to discuss the evidence behind interventions targeting these modifiable risk factors. Sleep disruption is associated with postoperative delirium, but the benefit of sleep-related interventions is uncertain. Pain is a risk factor for postoperative delirium, but its impact on other postoperative neurocognitive disorders is unknown. Multimodal analgesia and opioid avoidance are emerging as best practices, but data supporting their efficacy to prevent delirium are limited. Poor preoperative cognitive function is a strong predictor of postoperative neurocognitive disorder, and work is ongoing to determine whether it can be modified to prevent perioperative neurocognitive disorders.
预防围手术期神经认知障碍是患者、家属、临床医生和研究人员的首要任务。鉴于围手术期存在多种风险因素,多组分预防方法可能最有效。本叙述性综述的目的是强调睡眠、疼痛和认知对围手术期神经认知障碍风险的重要性,并讨论针对这些可改变风险因素的干预措施的证据。睡眠中断与术后谵妄有关,但睡眠相关干预的益处尚不确定。疼痛是术后谵妄的一个危险因素,但它对其他术后神经认知障碍的影响尚不清楚。多模式镇痛和避免使用阿片类药物正成为最佳实践,但支持其预防谵妄功效的数据有限。术前认知功能差是术后神经认知障碍的一个强有力预测因素,目前正在努力确定是否可以对其进行修改以预防围手术期神经认知障碍。