Gao Lei, Lim Andrew S P, Wong Patricia M, Gaba Arlen, Cui Longchang, Yu Lei, Buchman Aron S, Bennett David A, Hu Kun, Li Peng
Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USA.
Division of Sleep and Circadian Disorders, Brigham and Women's Hospital, Boston, MA 02115, USA.
Nat Sci Sleep. 2020 May 27;12:299-307. doi: 10.2147/NSS.S253757. eCollection 2020.
Heart failure has previously been linked to sleep disorders that are often associated with frequent disturbances to human rest/activity patterns. We tested whether fragmentation of sustained rest/activity patterns derived from actigraphic recordings at baseline predicts incident heart failure in community-based elderly individuals.
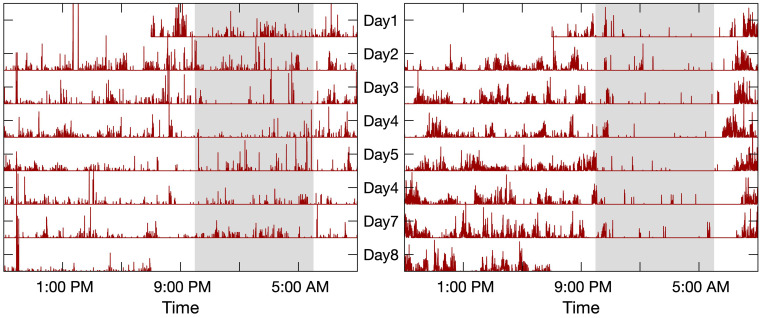
We studied 1099 community-based elderly adults participating in the Rush Memory and Aging Project who had baseline motor activity monitoring up to 11 days and were followed annually for up to 14 years. Fragmentation was assessed using previously validated indexes, derived from the probability of transitions once sustained rest or activity has been established. Heart failure was recorded via a clinical interview during the annual follow-up. Cox proportional hazards models were constructed to examine the relationship between rest fragmentation index and incident heart failure. Covariates grouped in terms of demographics, lifestyle factors and co-morbidities and cardiovascular risk factors/diseases were included.
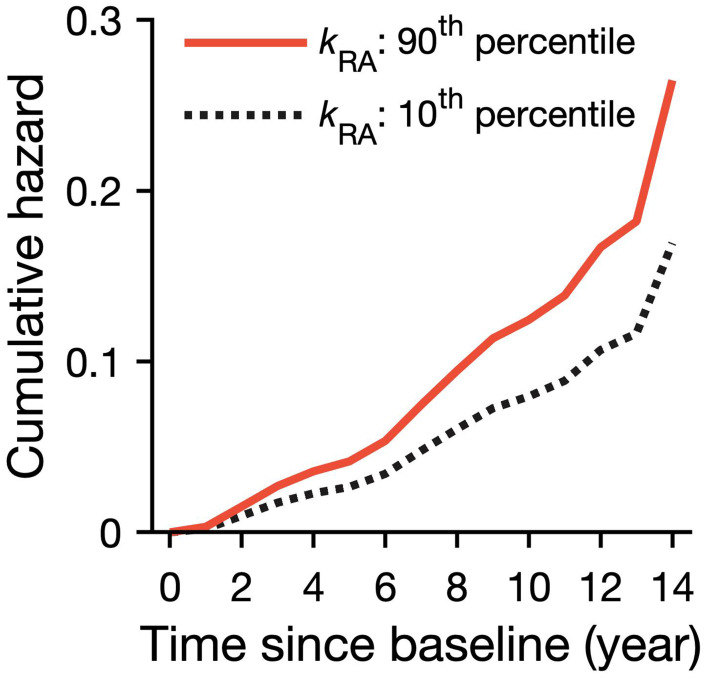
Increased rest fragmentation (but not activity fragmentation) was associated with higher risk for incident heart failure. Specifically, a subject with a rest fragmentation at the 90th percentile showed a 57% increased risk of developing incident heart failure compared to a subject at the 10th percentile in this cohort. This effect was equivalent to that of being over a decade older. These observations were consistent after adjusting for all covariates.
Increased rest fragmentation, a potential surrogate for sleep fragmentation, is independently associated with a higher risk of developing heart failure in community-based elderly adults during up to 14 years of follow-up. Further work is required to examine the specific contributions from daytime napping versus nighttime sleep periods in the elderly, as well as the underlying autonomic and cardio-dynamic pathways that may explain the effects on heart function.
心力衰竭此前已与睡眠障碍相关联,而睡眠障碍通常与人类休息/活动模式的频繁干扰有关。我们测试了基于基线活动记录仪记录得出的持续休息/活动模式碎片化是否能预测社区老年个体发生心力衰竭的情况。
我们研究了1099名参与拉什记忆与衰老项目的社区老年成年人,他们在基线时进行了长达11天的运动活动监测,并每年随访长达14年。使用先前验证的指标评估碎片化程度,该指标源自持续休息或活动建立后转换的概率。通过年度随访期间的临床访谈记录心力衰竭情况。构建Cox比例风险模型以检查休息碎片化指数与心力衰竭发生率之间的关系。纳入了根据人口统计学、生活方式因素、合并症以及心血管危险因素/疾病分组的协变量。
休息碎片化增加(而非活动碎片化增加)与发生心力衰竭的较高风险相关。具体而言,在该队列中,休息碎片化处于第90百分位的受试者发生心力衰竭的风险比处于第10百分位的受试者高57%。这种影响等同于年龄超过十岁的影响。在对所有协变量进行调整后,这些观察结果仍然一致。
休息碎片化增加,这是睡眠碎片化的一个潜在替代指标,在长达14年的随访期间,与社区老年成年人发生心力衰竭的较高风险独立相关。需要进一步开展工作,以研究老年人白天小睡与夜间睡眠时间的具体贡献,以及可能解释对心脏功能影响的潜在自主神经和心脏动力学途径。