Lancet Infect Dis. 2020 Jan;20(1):60-79. doi: 10.1016/S1473-3099(19)30410-4. Epub 2019 Oct 31.
Despite large reductions in under-5 lower respiratory infection (LRI) mortality in many locations, the pace of progress for LRIs has generally lagged behind that of other childhood infectious diseases. To better inform programmes and policies focused on preventing and treating LRIs, we assessed the contributions and patterns of risk factor attribution, intervention coverage, and sociodemographic development in 195 countries and territories by drawing from the Global Burden of Diseases, Injuries, and Risk Factors Study 2017 (GBD 2017) LRI estimates.
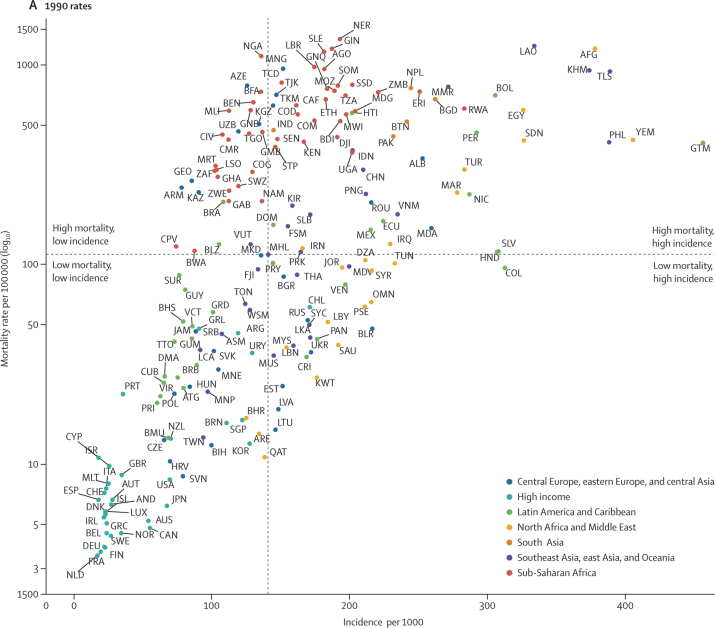
We used four strategies to model LRI burden: the mortality due to LRIs was modelled using vital registration data, demographic surveillance data, and verbal autopsy data in a predictive ensemble modelling tool; the incidence of LRIs was modelled using population representative surveys, health-care utilisation data, and scientific literature in a compartmental meta-regression tool; the attribution of risk factors for LRI mortality was modelled in a counterfactual framework; and trends in LRI mortality were analysed applying changes in exposure to risk factors over time. In GBD, infectious disease mortality, including that due to LRI, is among HIV-negative individuals. We categorised locations based on their burden in 1990 to make comparisons in the changing burden between 1990 and 2017 and evaluate the relative percent change in mortality rate, incidence, and risk factor exposure to explain differences in the health loss associated with LRIs among children younger than 5 years.
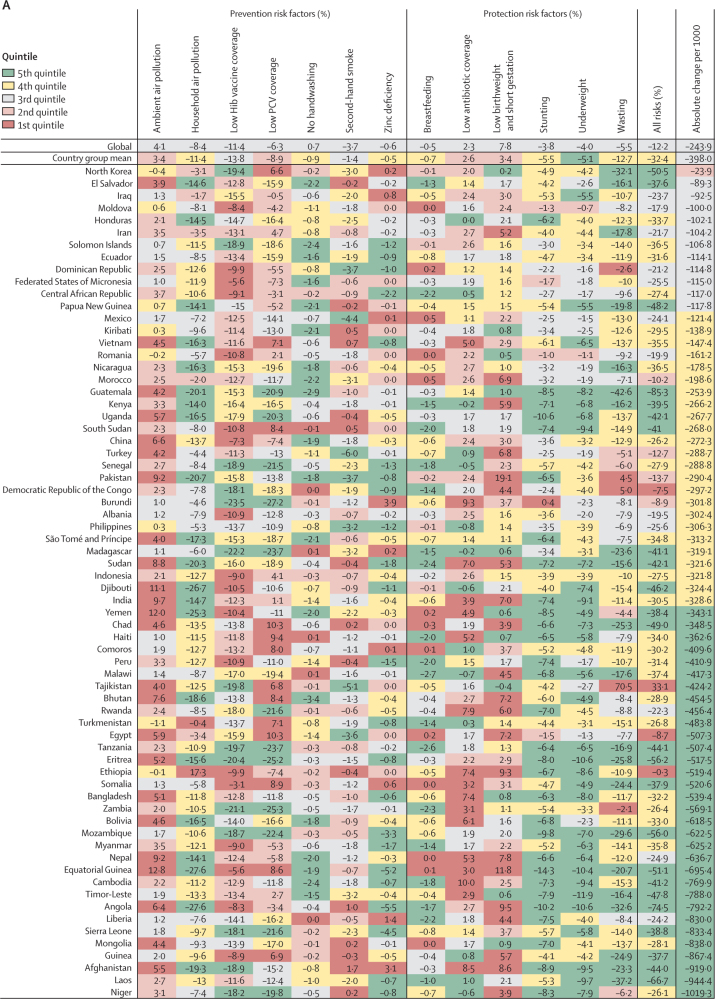
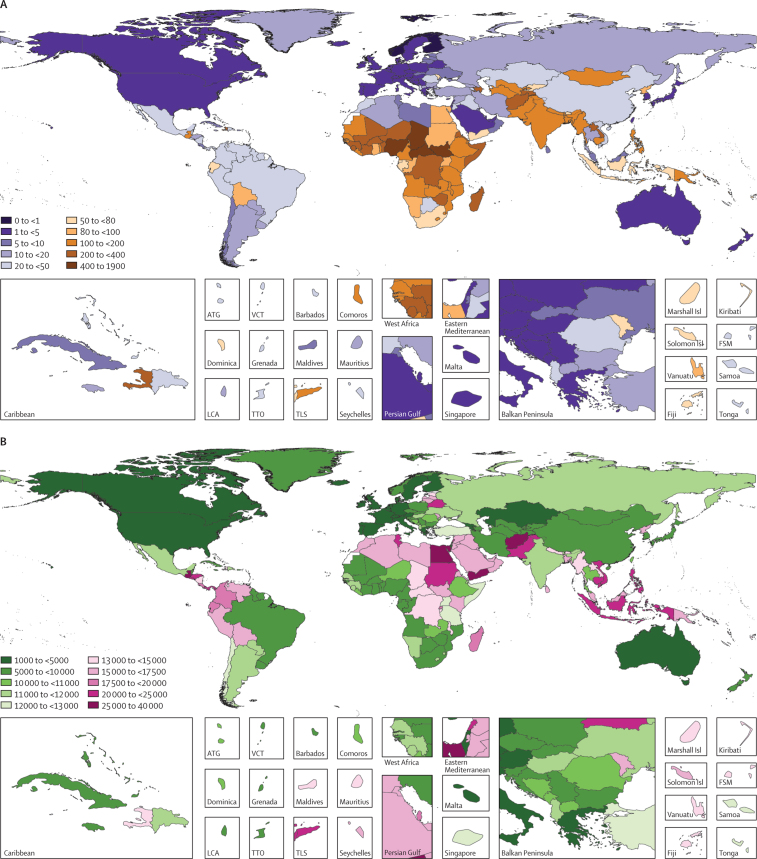
In 2017, LRIs caused 808 920 deaths (95% uncertainty interval 747 286-873 591) in children younger than 5 years. Since 1990, there has been a substantial decrease in the number of deaths (from 2 337 538 to 808 920 deaths; 65·4% decrease, 61·5-68·5) and in mortality rate (from 362·7 deaths [330·1-392·0] per 100 000 children to 118·9 deaths [109·8-128·3] per 100 000 children; 67·2% decrease, 63·5-70·1). LRI incidence declined globally (32·4% decrease, 27·2-37·5). The percent change in under-5 mortality rate and incidence has varied across locations. Among the risk factors assessed in this study, those responsible for the greatest decrease in under-5 LRI mortality between 1990 and 2017 were increased coverage of vaccination against Haemophilus influenza type b (11·4% decrease, 0·0-24·5), increased pneumococcal vaccine coverage (6·3% decrease, 6·1-6·3), and reductions in household air pollution (8·4%, 6·8-9·2).
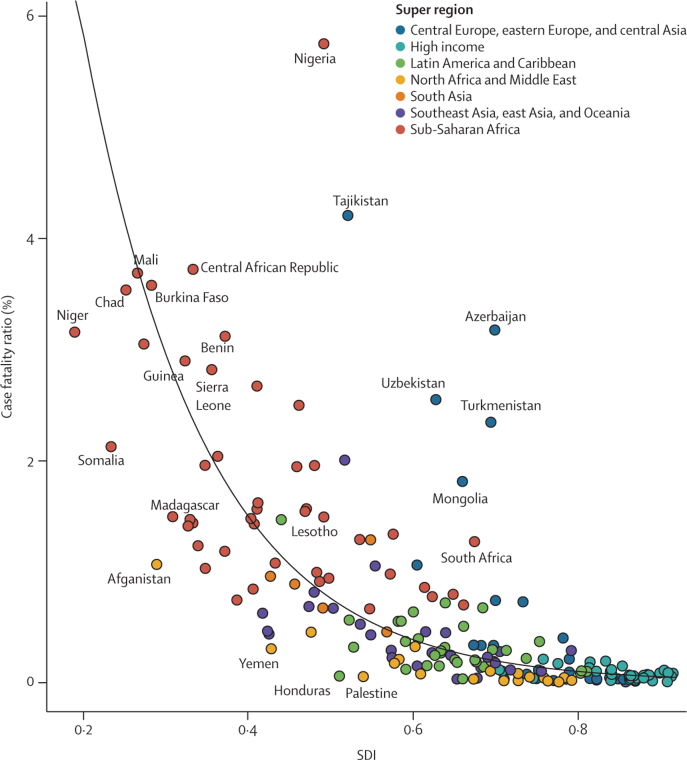
Our findings show that there have been substantial but uneven declines in LRI mortality among countries between 1990 and 2017. Although improvements in indicators of sociodemographic development could explain some of these trends, changes in exposure to modifiable risk factors are related to the rates of decline in LRI mortality. No single intervention would universally accelerate reductions in health loss associated with LRIs in all settings, but emphasising the most dominant risk factors, particularly in countries with high case fatality, can contribute to the reduction of preventable deaths.
Bill & Melinda Gates Foundation.
尽管在许多地方,5 岁以下下呼吸道感染(LRI)的死亡率大幅下降,但 LRI 的进展速度总体上落后于其他儿童传染病。为了更好地为预防和治疗 LRI 的项目和政策提供信息,我们利用 2017 年全球疾病、伤害和风险因素研究(GBD 2017)的 LRI 估计数据,从全球 195 个国家和地区评估了危险因素归因、干预措施覆盖范围和社会人口发展的贡献和模式。
我们使用了四种策略来建模 LRI 负担:通过预测性综合建模工具,使用生命登记数据、人口监测数据和死因推断数据来建模 LRI 死亡率;使用人口代表性调查、卫生保健利用数据和科学文献在隔室元回归工具中建模 LRI 发病率;在反事实框架中建模 LRI 死亡率的危险因素归因;并通过随时间变化的风险因素暴露情况分析 LRI 死亡率的趋势。在 GBD 中,包括 LRI 在内的传染病死亡率是针对 HIV 阴性个体的。我们根据 1990 年的负担对地点进行了分类,以便在 1990 年至 2017 年之间的变化负担中进行比较,并评估死亡率、发病率和风险因素暴露的相对百分比变化,以解释 5 岁以下儿童与 LRI 相关的健康损失的差异。
2017 年,5 岁以下儿童的 LRI 导致 808920 人死亡(95%置信区间 747286-873591)。自 1990 年以来,死亡人数(从 2337538 人减少到 808920 人;减少 65.4%,61.5-68.5)和死亡率(从每 100000 名儿童 362.7 人死亡[330.1-392.0]减少到每 100000 名儿童 118.9 人死亡[109.8-128.3];减少 67.2%,63.5-70.1)大幅下降。LRI 发病率在全球范围内下降(下降 32.4%,27.2-37.5)。地点之间的 5 岁以下死亡率和发病率的变化百分比有所不同。在本研究评估的危险因素中,导致 1990 年至 2017 年期间 5 岁以下 LRI 死亡率下降幅度最大的是增加针对流感嗜血杆菌 b 型的疫苗接种覆盖率(下降 11.4%,0.0-24.5)、增加肺炎球菌疫苗覆盖率(下降 6.3%,6.1-6.3)和减少家庭空气污染(下降 8.4%,6.8-9.2)。
我们的研究结果表明,1990 年至 2017 年期间,各国的 LRI 死亡率有了实质性但不平衡的下降。尽管社会人口发展指标的改善可以解释其中的一些趋势,但可改变风险因素暴露的变化与 LRI 死亡率的下降率有关。没有单一的干预措施可以在所有情况下普遍加速与 LRI 相关的健康损失的减少,但强调最主要的危险因素,特别是在病死率高的国家,可以有助于减少可预防的死亡。
比尔和梅琳达·盖茨基金会。