Torres-Macho Juan, Sánchez-Fernández Marcos, Arnanz-González Irene, Tung-Chen Yale, Franco-Moreno Ana Isabel, Duffort-Falcó Mercedes, Beltrán-Romero Luis, Rodríguez-Suaréz Santiago, Bernabeu-Wittel Máximo, Urbano Elena, Méndez-Bailon Manuel, Roque-Rojas Fernando, García-Guijarro Elena, García-Casasola Gonzalo
Internal Medicine Department, Infanta Leonor-Virgen de la Torre University Hospital, 28031 Madrid, Spain.
Department of Medicine, School of Medicine, Complutense University, 28040 Madrid, Spain.
J Clin Med. 2021 Oct 20;10(21):4818. doi: 10.3390/jcm10214818.
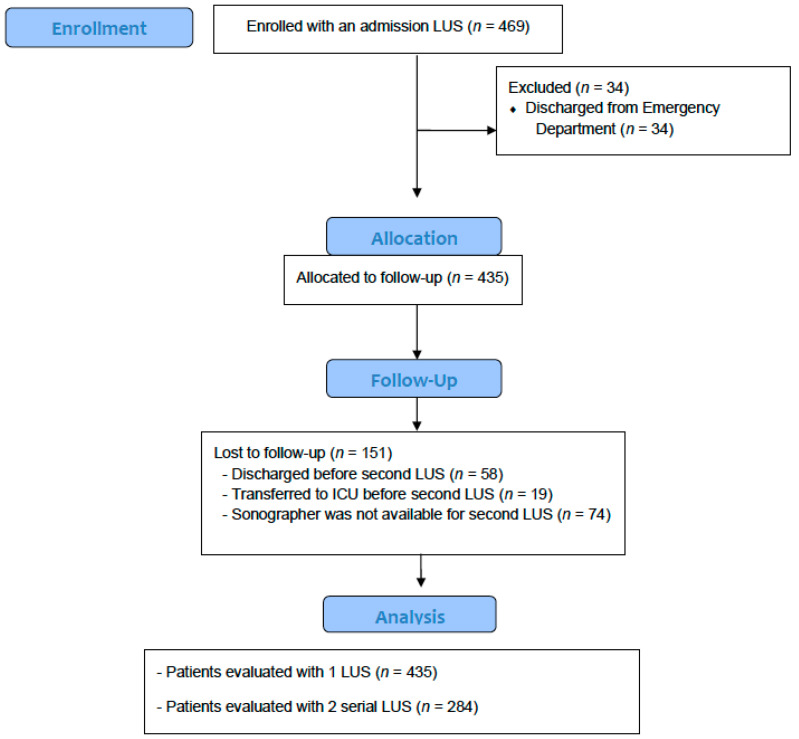
The value of serial lung ultrasound (LUS) in patients with COVID-19 is not well defined. In this multicenter prospective observational study, we aimed to assess the prognostic accuracy of serial LUS in patients admitted to hospital due to COVID-19. The serial LUS protocol included two examinations (0-48 h and 72-96 h after admission) using a 10-zones sequence, and a 0 to 5 severity score. Primary combined endpoint was death or the need for invasive mechanical ventilation. Calibration (Hosmer-Lemeshow test and calibration curves), and discrimination power (area under the ROC curve) of both ultrasound exams (SCORE1 and 2), and their difference (DIFFERENTIAL-SCORE) were performed. A total of 469 patients (54.2% women, median age 60 years) were included. The primary endpoint occurred in 51 patients (10.9%). Probability risk tertiles of SCORE1 and SCORE2 (0-11 points, 12-24 points, and ≥25 points) obtained a high calibration. SCORE-2 showed a higher discrimination power than SCORE-1 (AUC 0.72 (0.58-0.85) vs. 0.61 (0.52-0.7)). The DIFFERENTIAL-SCORE showed a higher discrimination power than SCORE-1 and SCORE-2 (AUC 0.78 (0.66-0.9)). An algorithm for clinical decision-making is proposed. Serial lung ultrasound performing two examinations during the first days of hospitalization is an accurate strategy for predicting clinical deterioration of patients with COVID-19.
连续肺部超声(LUS)在新型冠状病毒肺炎(COVID-19)患者中的价值尚未明确。在这项多中心前瞻性观察研究中,我们旨在评估因COVID-19入院患者连续LUS的预后准确性。连续LUS方案包括使用10区序列进行两次检查(入院后0 - 48小时和72 - 96小时),以及0至5的严重程度评分。主要联合终点是死亡或需要有创机械通气。对两次超声检查(SCORE1和2)及其差值(DIFFERENTIAL - SCORE)进行校准(Hosmer - Lemeshow检验和校准曲线)以及鉴别力(ROC曲线下面积)分析。共纳入469例患者(女性占54.2%,中位年龄60岁)。51例患者(10.9%)出现主要终点。SCORE1和SCORE2的概率风险三分位数(0 - 11分、12 - 24分和≥25分)校准良好。SCORE - 2的鉴别力高于SCORE - 1(AUC 0.72(0.58 - 0.85)对0.61(0.52 - 0.7))。DIFFERENTIAL - SCORE的鉴别力高于SCORE - 1和SCORE - 2(AUC 0.78(0.66 - 0.9))。提出了一种临床决策算法。在住院的头几天进行两次检查的连续肺部超声是预测COVID-19患者临床恶化的准确策略。