Sun Yuxi, Si Jinping, Li Jiaxin, Dai Mengyuan, King Emma, Zhang Xinxin, Zhang Yanli, Xia Yunlong, Tse Gary, Liu Ying
Heart Failure and Structural Cardiology Ward, First Affiliated Hospital of Dalian Medical University, Dalian, China.
Cardiovascular Analytics Group, Hong Kong SAR, China.
Front Cardiovasc Med. 2021 Oct 29;8:656536. doi: 10.3389/fcvm.2021.656536. eCollection 2021.
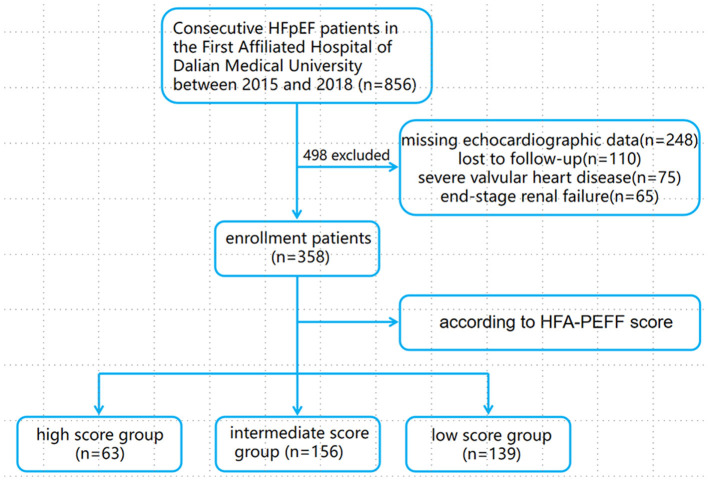
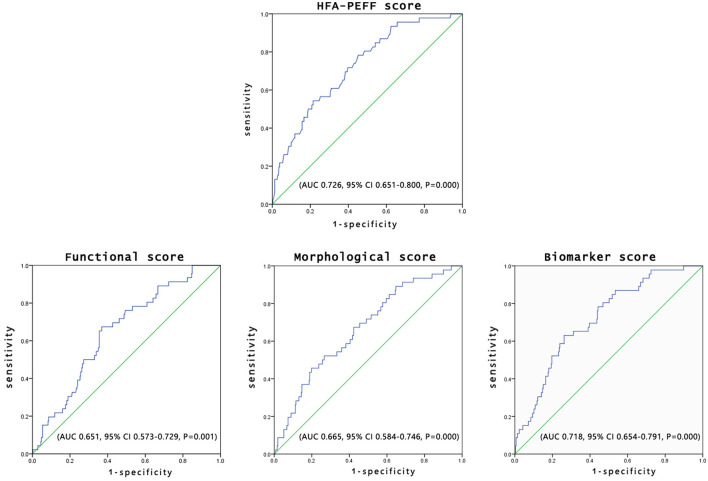
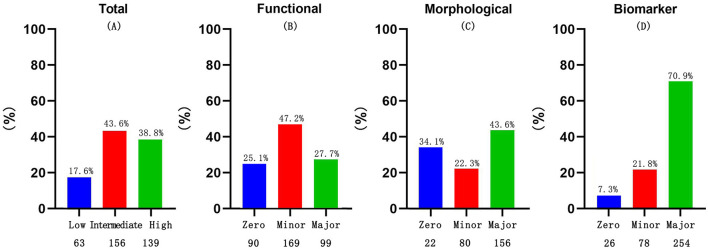
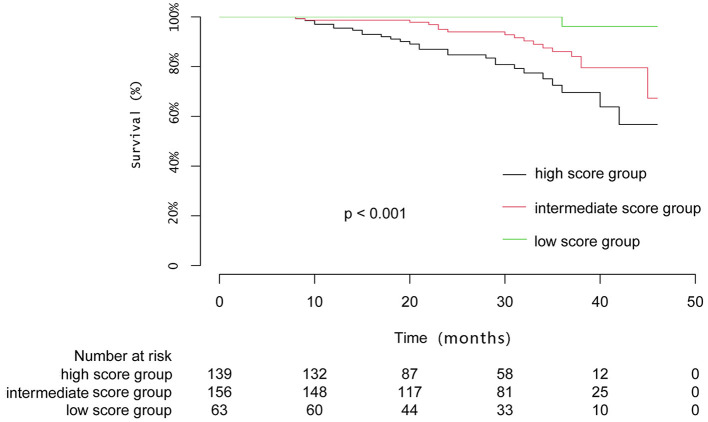
HFA-PEFF score has been proposed for diagnosing heart failure with preserved ejection fraction (HFpEF). Currently, there are only a limited number of tools for predicting the prognosis. In this study, we evaluated whether the HFA-PEFF score can predict mortality in patients with HFpEF. This single-center, retrospective observational study enrolled patients diagnosed with HFpEF at the First Affiliated Hospital of Dalian Medical University between January 1, 2015, and April 30, 2018. The subjects were divided according to their HFA-PEFF score into low (0-2 points), intermediate (3-4 points), and high (5-6 points) score groups. The primary outcome was all-cause mortality. A total of 358 patients (mean age: 70.21 ± 8.64 years, 58.1% female) were included. Of these, 63 (17.6%), 156 (43.6%), and 139 (38.8%) were classified into the low, intermediate, and high score groups, respectively. Over a mean follow-up of 26.9 months, 46 patients (12.8%) died. The percentage of patients who died in the low, intermediate, and high score groups were 1 (1.6%), 18 (11.5%), and 27 (19.4%), respectively. A multivariate Cox regression identified HFA-PEFF score as an independent predictor of all-cause mortality [hazard ratio ():1.314, 95% : 1.013-1.705, = 0.039]. A Cox analysis demonstrated a significantly higher rate of mortality in the intermediate (: 4.912, 95% 1.154-20.907, = 0.031) and high score groups (: 5.291, 95% : 1.239-22.593, = 0.024) than the low score group. A receiver operating characteristic (ROC) analysis indicated that the HFA-PEFF score can effectively predict all-cause mortality after adjusting for age and New York Heart Association (NYHA) class [area under the curve (AUC) 0.726, 95% 0.651-0.800, = 0.000]. With an HFA-PEFF score cut-off value of 3.5, the sensitivity and specificity were 78.3 and 54.8%, respectively. The AUC on ROC analysis for the biomarker component of the score was similar to that of the total score. The HFA-PEFF score can be used both to diagnose HFpEF and predict the prognosis. The higher scores are associated with higher all-cause mortality.
HFA-PEFF评分已被用于诊断射血分数保留的心力衰竭(HFpEF)。目前,预测预后的工具数量有限。在本研究中,我们评估了HFA-PEFF评分是否能够预测HFpEF患者的死亡率。这项单中心回顾性观察研究纳入了2015年1月1日至2018年4月30日期间在大连医科大学附属第一医院被诊断为HFpEF的患者。根据HFA-PEFF评分将受试者分为低(0-2分)、中(3-4分)、高(5-6分)评分组。主要结局是全因死亡率。共纳入358例患者(平均年龄:70.21±8.64岁,58.1%为女性)。其中,63例(17.6%)、156例(43.6%)和139例(38.8%)分别被归入低、中、高评分组。在平均26.9个月的随访期内,46例患者(12.8%)死亡。低、中、高评分组患者的死亡百分比分别为1例(1.6%)、18例(11.5%)和27例(19.4%)。多因素Cox回归分析确定HFA-PEFF评分为全因死亡率的独立预测因子[风险比(HR):1.314,95%置信区间(CI):1.013-1.705,P = 0.039]。Cox分析表明,中评分组(HR:4.912,95%CI:1.154-20.907,P = 0.031)和高评分组(HR:5.291,95%CI:1.239-22.593,P = 0.024)的死亡率显著高于低评分组。受试者工作特征(ROC)分析表明,在调整年龄和纽约心脏协会(NYHA)心功能分级后,HFA-PEFF评分能够有效预测全因死亡率[曲线下面积(AUC)为0.726,95%CI:0.651-0.800,P = 0.000]。HFA-PEFF评分的截断值为3.5时,敏感性和特异性分别为78.3%和54.8%。该评分生物标志物成分的ROC分析AUC与总分的AUC相似。HFA-PEFF评分可用于诊断HFpEF并预测预后。评分越高,全因死亡率越高。