Luo Zai, Fu Zhongmao, Li Tengfei, Zhang Yuan, Zhang Jianming, Yang Yan, Yang Zhengfeng, Li Qi, Qiu Zhengjun, Huang Chen
Department of Gastrointestinal Surgery, Shanghai General Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Institute of Translational Medicine, Shanghai General Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Front Oncol. 2021 Nov 1;11:709835. doi: 10.3389/fonc.2021.709835. eCollection 2021.
The overall survival (OS) of patients diagnosed with colon cancer (CC) varied greatly, so did the patients with the same tumor stage. We aimed to design a nomogram that is capable of predicting OS in resected left-sided colon cancers (LSCC) and right-sided colon cancers (RSCC), and thus to stratify patients into different risk groups, respectively.
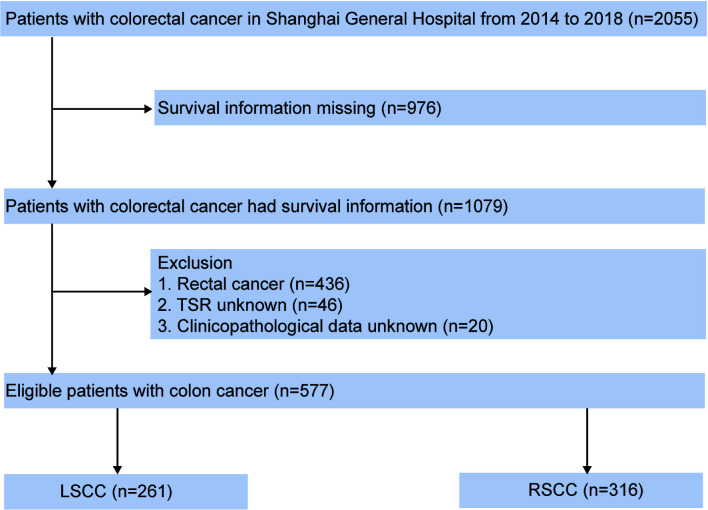
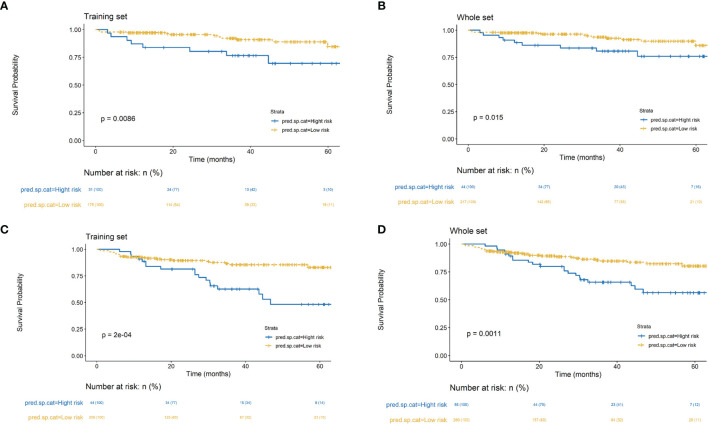
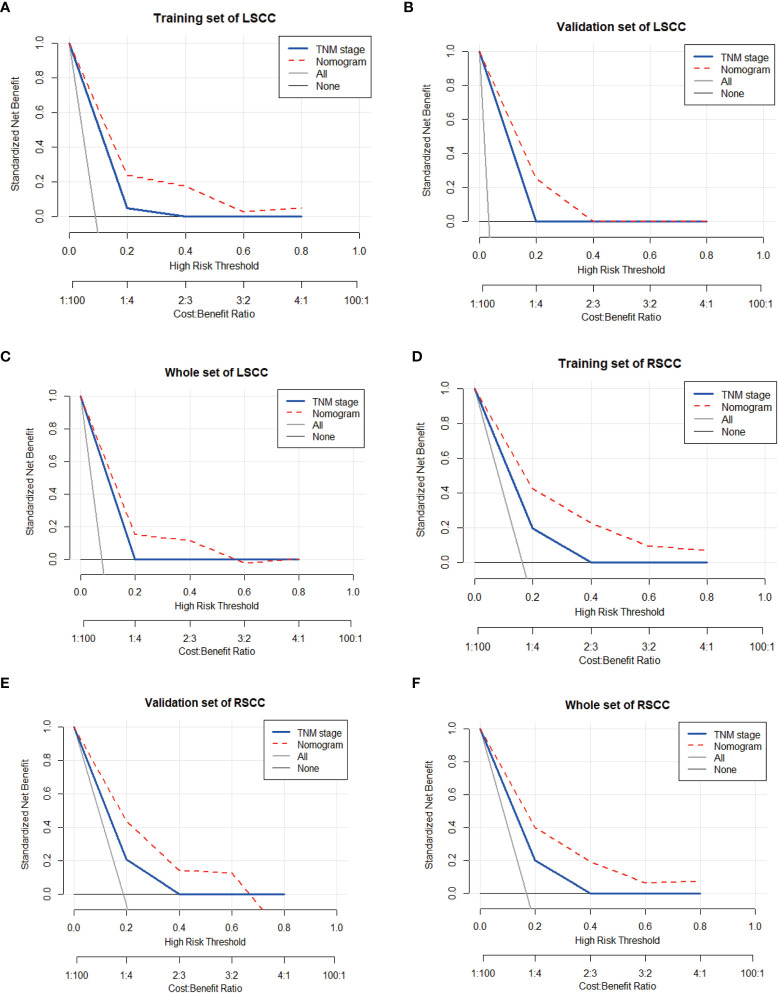
Records from a retrospective cohort of 577 patients with complete information were used to construct the nomogram. Univariate and multivariate analyses screened risk factors associated with overall survival. The performance of the nomogram was evaluated with concordance index (c-index), calibration plots, and decision curve analyses for discrimination, accuracy, calibration ability, and clinical net benefits, respectively, which was further compared with the American Joint Committee on Cancer (AJCC) 8th tumor-node-metastasis (TNM) classification. Risk stratification based on nomogram scores was performed with recursive partitioning analysis.
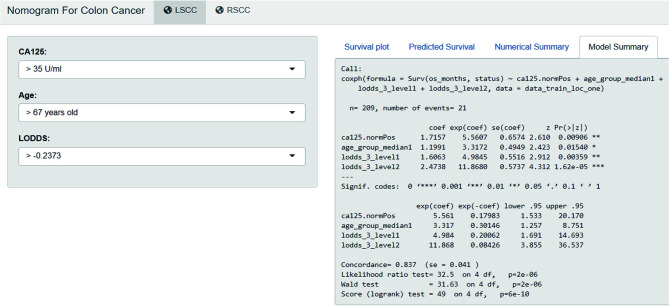
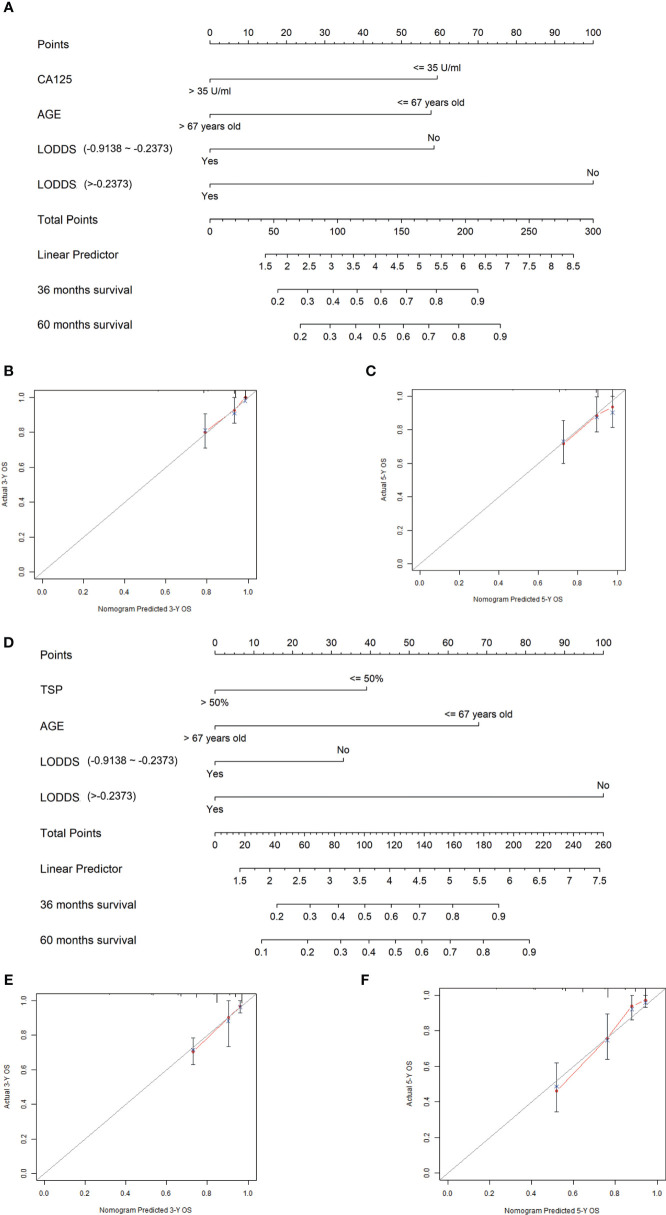
The LSCC nomogram incorporated carbohydrate antigen 12-5 (CA12-5), age and log odds of positive lymph nodes (LODDS), and RSCC nomogram enrolled tumor stroma percentage (TSP), age and LODDS. Compared with the TNM classification, the LSCC and RSCC nomograms both had a statistically higher C-index (0.837, 95% CI: 0.827-0.846 and 0.780, 95% CI 0.773-0.787, respectively) and more clinical net benefits, respectively. Calibration plots revealed no deviations from reference lines. All results were reproducible in the validation cohort.
An original predictive nomogram was constructed and validated for OS in patients with CC after surgery, which had facilitated physicians to appraise the individual survival of postoperative patients accurately and to identify high-risk patients who were in need of more aggressive treatment and follow-up strategies.
结肠癌(CC)患者的总生存期(OS)差异很大,处于相同肿瘤分期的患者也是如此。我们旨在设计一种列线图,能够预测接受手术切除的左侧结肠癌(LSCC)和右侧结肠癌(RSCC)患者的OS,并据此将患者分别分为不同的风险组。
来自577例具有完整信息的回顾性队列研究记录用于构建列线图。单因素和多因素分析筛选与总生存期相关的危险因素。分别使用一致性指数(c指数)、校准曲线和决策曲线分析评估列线图在区分度、准确性、校准能力和临床净获益方面的性能,并与美国癌症联合委员会(AJCC)第8版肿瘤-淋巴结-转移(TNM)分类进行进一步比较。基于列线图评分进行风险分层,采用递归划分分析。
LSCC列线图纳入了糖类抗原12-5(CA12-5)、年龄和阳性淋巴结对数优势比(LODDS),RSCC列线图纳入了肿瘤间质百分比(TSP)、年龄和LODDS。与TNM分类相比,LSCC和RSCC列线图的C指数均在统计学上更高(分别为0.837,95%CI:0.827-0.846和0.780,95%CI:0.773-0.787),且临床净获益更多。校准曲线显示与参考线无偏差。所有结果在验证队列中均可重复。
构建并验证了一种用于CC患者术后OS的原创性预测列线图,有助于医生准确评估术后患者的个体生存期,并识别需要更积极治疗和随访策略的高危患者。