Kundi Harun, Coskun Nazim, Yesiltepe Metin
Department of Cardiology, Ankara City Hospital, Ankara, Turkey.
Department of Digital Hospital and Analytical Management Unit, Ankara City Hospital, Ankara, Turkey.
Lancet Reg Health Eur. 2021 Jul 29;10:100183. doi: 10.1016/j.lanepe.2021.100183. eCollection 2021 Nov.
Several countries have increasingly focused on improving care for acute myocardial infarction (AMI), heart failure (HF), and pneumonia to reduce their readmissions and mortality rates. Frailty is becoming increasingly important to accurately predict healthcare utilization for the aging population. The preferred method for the measurement of frailty remains unclear, and current risk-adjustment models do not account for frailty. We sought to compare commonly used frailty indices in terms of the ability to predict clinical adverse outcomes in AMI, HF, and pneumonia patients.
A nationwide cohort study included AMI, HF, and pneumonia with 65 years and older patients in the Turkey between January 1 and December 31, 2018. The primary predictor of interest was frailty. We used two claims-based frailty indices (Johns Hopkins Claims-Based Frailty Index and Hospital Frailty Risk Score) to assess frailty. The main outcome was all-cause long-term mortality up to 3 years. Time to death was calculated as the time period between the date of first admission and the date of death. Patients were censored as of September 30, 2020, which marked the end of the follow-up period.
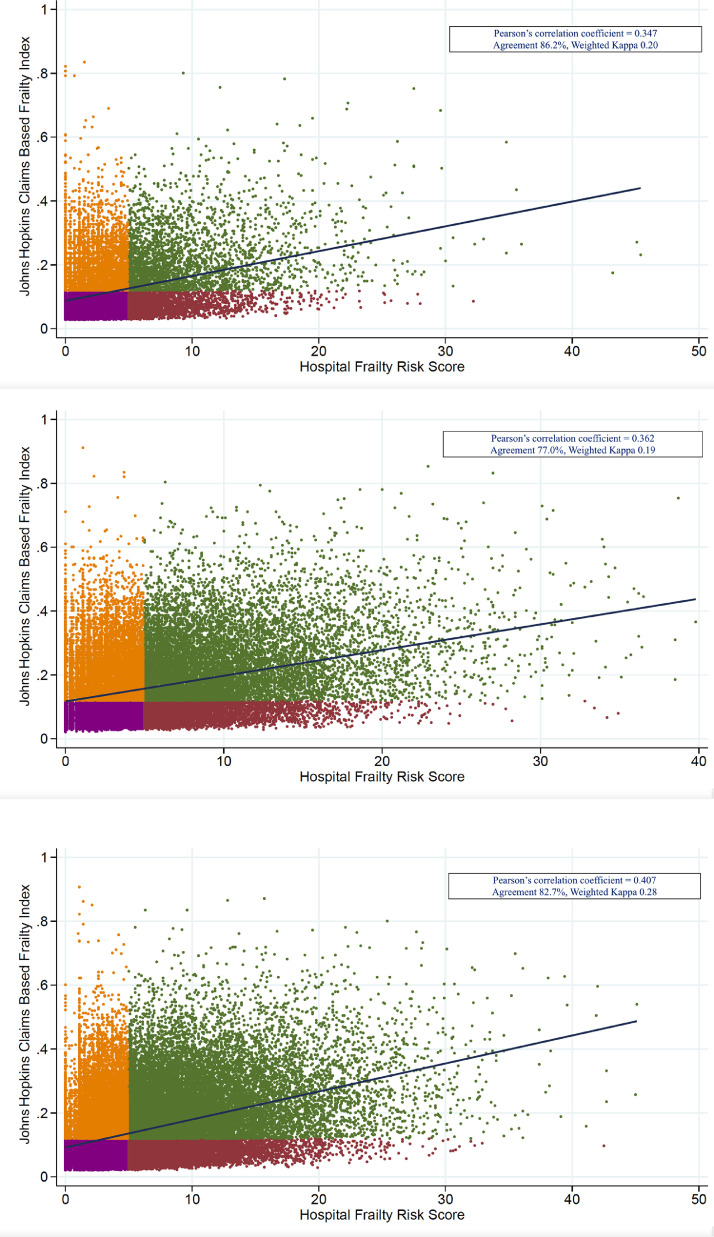
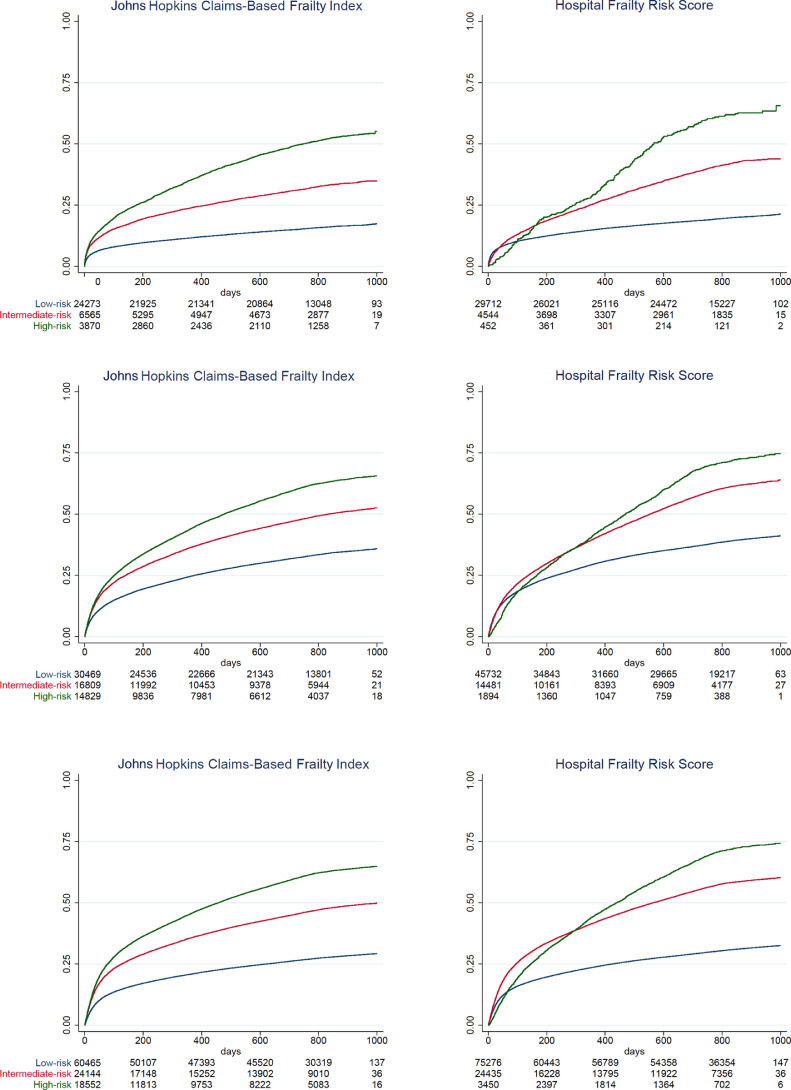
Of the 200,948 patients, 35,096 (17.5%) had AMI, 62,403 (31.1%) had HF, and 103,449 (51.5%) had pneumonia. Johns Hopkins Claims-Based Frailty Index (c-statistics for long-term mortality: 0.68 in AMI, 0.61 in HF, 0.64 in pneumonia) was better compared to Hospital Frailty Risk Score (c-statistics for long-term mortality: AMI=0.62, HF=0.58, pneumonia=0.62) (DeLong p<0.001 in all).
Readmission and mortality rates after AMI, HF, and pneumonia gradually increases with increasing frailty score. While the Hospital Frailty Risk Score had a better discrimination for predicting readmissions, Johns Hopkins Claims-Based Frailty Index had a better discrimination for predicting mortality. These findings should be taken into account for a better evaluation of hospital performance.
This study was supported by funding from The Scientific and Technological Research Council of Turkey (grant 120S422, HK).
一些国家越来越关注改善急性心肌梗死(AMI)、心力衰竭(HF)和肺炎的护理,以降低再入院率和死亡率。衰弱对于准确预测老年人群的医疗服务利用情况变得越来越重要。衰弱测量的首选方法仍不明确,并且当前的风险调整模型未考虑衰弱因素。我们试图比较常用的衰弱指数在预测AMI、HF和肺炎患者临床不良结局方面的能力。
一项全国性队列研究纳入了2018年1月1日至12月31日期间土耳其65岁及以上患有AMI、HF和肺炎的患者。主要关注的预测因素是衰弱。我们使用了两种基于索赔数据的衰弱指数(约翰霍普金斯基于索赔数据的衰弱指数和医院衰弱风险评分)来评估衰弱。主要结局是长达3年的全因长期死亡率。死亡时间计算为首次入院日期与死亡日期之间的时间段。截至2020年9月30日对患者进行截尾,这标志着随访期结束。
在200948名患者中,35096名(17.5%)患有AMI,62403名(31.1%)患有HF,103449名(51.5%)患有肺炎。与医院衰弱风险评分(长期死亡率的c统计量:AMI = 0.62,HF = 0.58,肺炎 = 0.62)相比,约翰霍普金斯基于索赔数据的衰弱指数(长期死亡率的c统计量:AMI中为0.68,HF中为0.61,肺炎中为0.64)表现更好(所有比较中DeLong p < 0.001)。
AMI、HF和肺炎后的再入院率和死亡率随着衰弱评分的增加而逐渐升高。虽然医院衰弱风险评分在预测再入院方面具有更好的辨别力,但约翰霍普金斯基于索赔数据的衰弱指数在预测死亡率方面具有更好的辨别力。为了更好地评估医院绩效,应考虑这些发现。
本研究由土耳其科学技术研究理事会资助(资助编号120S422,HK)。