Institute of General Practice and Public Health, College of Health Care Professions, Lorenz Böhler- Street 13, 39100, Bolzano, Italy.
Institute of General Practice, Family Medicine and Preventive Medicine, Paracelsus Medical University, Strubergasse 21, 5020, Salzburg, Austria.
BMC Geriatr. 2021 Nov 23;21(1):659. doi: 10.1186/s12877-021-02612-0.
Evidence regarding clinically relevant effects of interventions aiming at reducing polypharmacy is weak, especially for the primary care setting. This study was initiated with the objective to achieve clinical benefits for older patients (aged 75+) by means of evidence-based reduction of polypharmacy (defined as ≥8 prescribed drugs) and inappropriate prescribing in general practice.
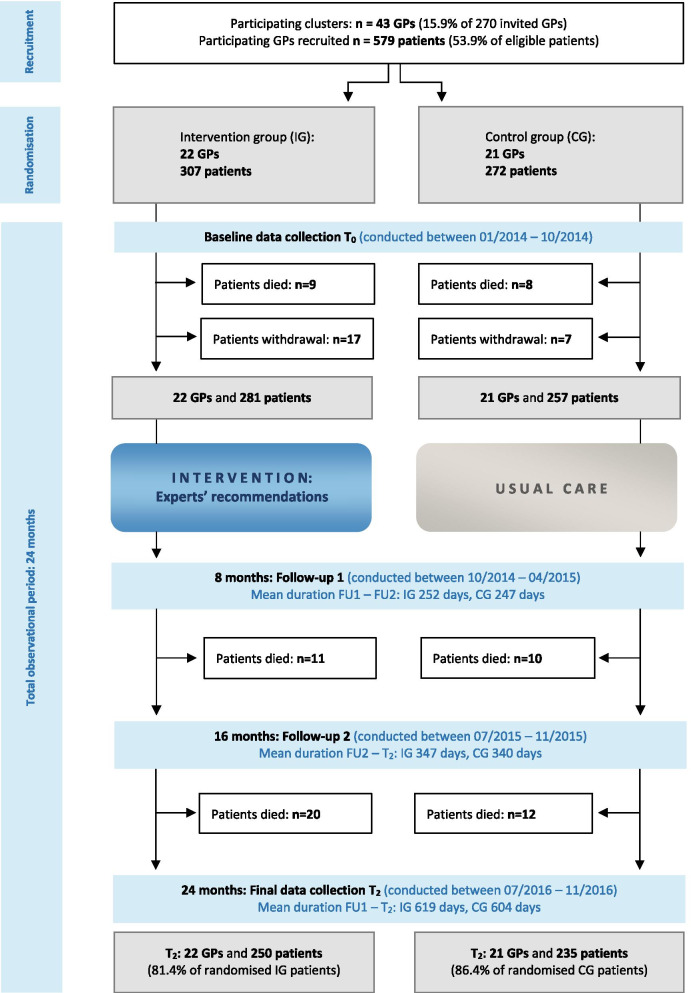
The cluster-randomised controlled trial involved general practitioners and patients in a northern-Italian region. The intervention consisted of a review of patient's medication regimens by three experts who gave specific recommendations for drug discontinuation. Main outcome measures were non-elective hospital admissions or death within 24 months (composite primary endpoint). Secondary outcomes were drug numbers, hospital admissions, mortality, falls, fractures, quality of life, affective status, cognitive function.
Twenty-two GPs/307 patients participated in the intervention group, 21 GPs/272 patients in the control group. One hundred twenty-five patients (40.7%) experienced the primary outcome in the intervention group, 87 patients (32.0%) in the control group. The adjusted rates of occurrence of the primary outcome did not differ significantly between the study groups (intention-to-treat analysis: adjusted odds ratio 1.46, 95%CI 0.99-2.18, p = 0.06; per-protocol analysis: adjusted OR 1.33, 95%CI 0.87-2.04, p = 0.2). Hospitalisations as single endpoint occurred more frequently in the intervention group according to the unadjusted analysis (OR 1.61, 95%CI 1.03-2.51, p = 0.04) but not in the adjusted analysis (OR 1.39, 95%CI 0.95-2.03, p = 0.09). Falls occurred less frequently in the intervention group (adjusted OR 0.55, 95%CI 0.31-0.98; p = 0.04). No significant differences were found regarding the other outcomes. Definitive discontinuation was obtained for 67 (16.0%) of 419 drugs rated as inappropriate. About 6% of the prescribed drugs were PIMs.
No conclusive effects were found regarding mortality and non-elective hospitalisations as composite respectively single endpoints. Falls were significantly reduced in the intervention group, although definitive discontinuation was achieved for only one out of six inappropriate drugs. These results indicate that (1) even a modest reduction of inappropriate medications may entail positive clinical effects, and that (2) focusing on evidence-based new drug prescriptions and prevention of polypharmacy may be more effective than deprescribing.
Current Controlled Trials (ID ISRCTN: 38449870), date: 11/09/2013.
旨在减少多种药物治疗的干预措施对临床相关效果的证据较弱,特别是在初级保健环境中。本研究的目的是通过循证减少老年人(75 岁以上)的多种药物治疗(定义为≥8 种处方药)和一般实践中的不适当处方来为老年患者带来临床益处。
这项基于群组的随机对照试验涉及意大利北部地区的全科医生和患者。该干预措施包括由三位专家对患者的药物治疗方案进行审查,并对停药提出具体建议。主要结局指标是 24 个月内非选择性住院或死亡(主要复合终点)。次要结局指标是药物数量、住院、死亡率、跌倒、骨折、生活质量、情感状态、认知功能。
22 名全科医生/307 名患者参加了干预组,21 名全科医生/272 名患者参加了对照组。干预组中有 125 名患者(40.7%)发生了主要结局,对照组中有 87 名患者(32.0%)。研究组之间主要结局的发生率无显著差异(意向治疗分析:调整后的优势比 1.46,95%CI 0.99-2.18,p=0.06;方案分析:调整后的 OR 1.33,95%CI 0.87-2.04,p=0.2)。根据未调整分析,干预组的住院治疗作为单一终点更为频繁(OR 1.61,95%CI 1.03-2.51,p=0.04),但在调整分析中则不然(OR 1.39,95%CI 0.95-2.03,p=0.09)。干预组跌倒发生的频率较低(调整后的 OR 0.55,95%CI 0.31-0.98;p=0.04)。其他结果无显著差异。419 种被评定为不适当的药物中,有 67 种(16.0%)被明确停用。处方药物中有约 6%是 PIMs。
未发现死亡率和非选择性住院作为复合或单一终点的明确效果。干预组的跌倒显著减少,尽管只有六分之一的不适当药物被明确停用。这些结果表明,(1)即使适度减少不适当的药物治疗也可能带来积极的临床效果,(2)关注基于证据的新药处方和预防多种药物治疗可能比停药更有效。
当前对照试验(ID ISRCTN:38449870),日期:2013 年 9 月 11 日。