Institute of Primary Care (IHAMZ), University and University Hospital of Zurich, Pestalozzistrasse 24, CH-8091, Zurich, Switzerland.
Institute of Primary Health Care (BIHAM), University of Bern, Bern, Switzerland.
Implement Sci. 2018 Dec 27;13(1):155. doi: 10.1186/s13012-018-0839-1.
Inappropriate medication and polypharmacy increase morbidity, hospitalisation rate, costs and mortality in multimorbid patients. At hospital discharge of elderly patients, polypharmacy is often even more pronounced than at admission. However, the optimal discharge strategy in view of sustained medication appropriateness remains unclear. In particular, unreflectingly switching back to the pre-hospitalisation medication must be avoided. Therefore, both the patients and the follow-up physicians should be involved in the discharge process. In this study, we aim to test whether a brief medication review which takes the patients' priorities into account, combined with a standardised communication strategy at hospital discharge, leads to sustained medication appropriateness and extends readmission times among elderly multimorbid patients.
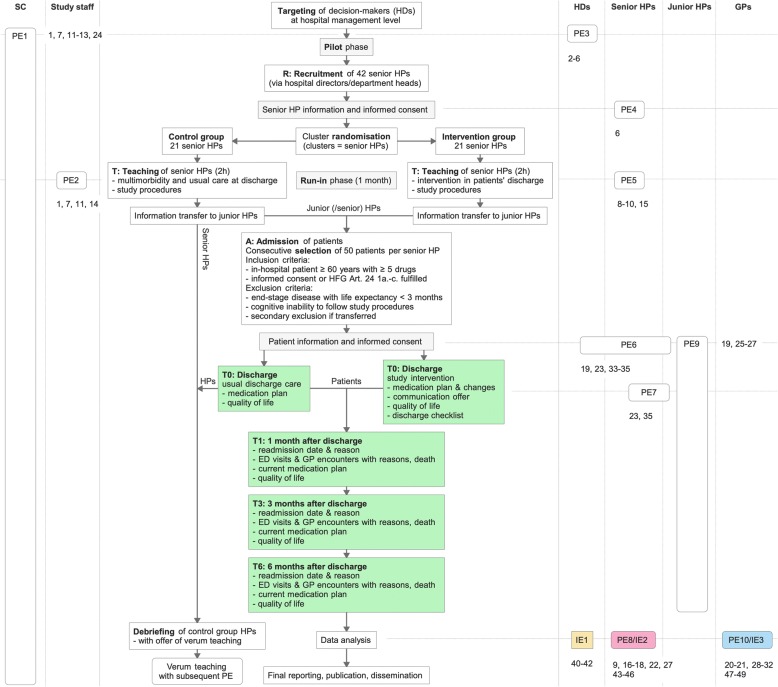
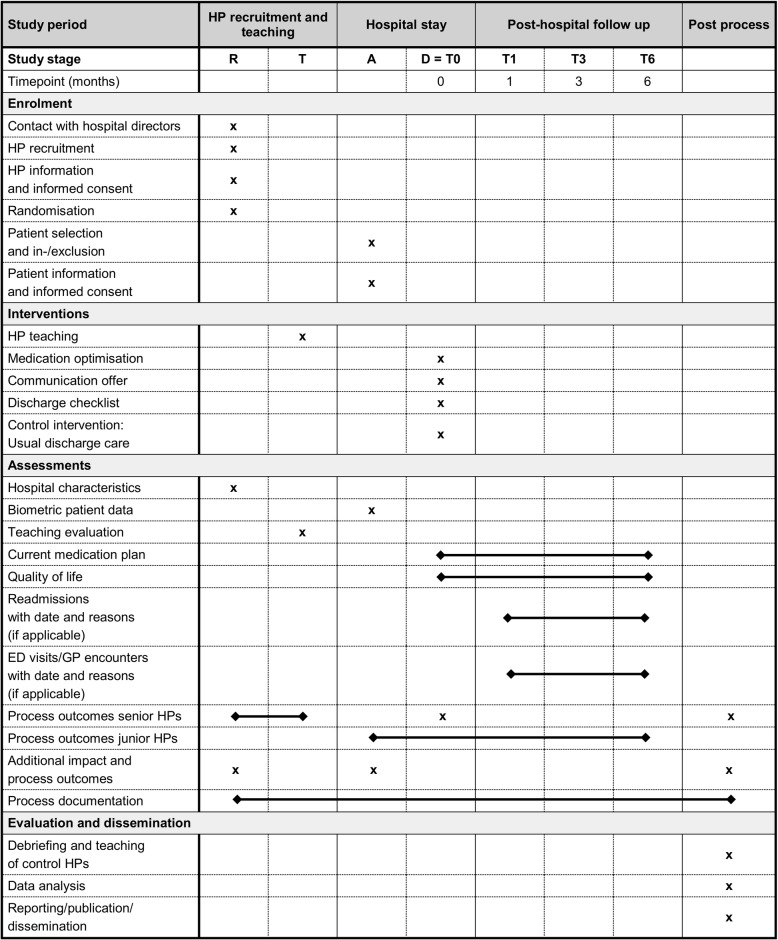
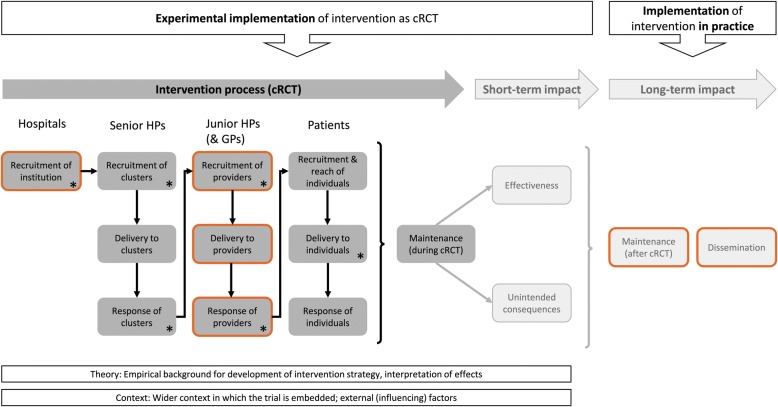
The study is designed as a two-armed, double-blinded, cluster-randomised trial, involving 42 senior hospital physicians (HPs) with their junior HPs and 2100 multimorbid patients aged 60 years or older. Using a randomised minimisation strategy, senior HPs will be assigned to either intervention or control group. Following instructions of the study team, the senior HPs in the intervention group will teach their junior HPs how to integrate a simple medication review tool combined with a defined communication strategy into their ward's discharge procedure. The untrained HPs in the control group will provide data on usual care, and their patients will be discharged following usual local routines. Primary outcome is the time until readmission within 6 months after discharge, and secondary outcomes cover readmission rates, number of emergency and GP visits, classes and numbers of drugs prescribed, proportions of potentially inappropriate medications, and the patients' quality of life after discharge. Additionally, the characteristics of both the HPs as well as the patients will be collected before the intervention. Process evaluation outcomes will be assessed parallel to the ongoing core study using qualitative research methods.
So far, interventions to reduce polypharmacy are still scarce at the crucial interface between HPs and GPs. To our knowledge, this trial is the first to analyse the combination of a brief deprescribing intervention with a standardised communication strategy at hospital discharge and in the early post-discharge period.
ISRCTN, ISRCTN18427377 . Registered 11 January 2018.
不适当的用药和多种药物治疗会增加多病患者的发病率、住院率、成本和死亡率。在老年患者出院时,多种药物治疗往往比入院时更为明显。然而,关于维持药物适当性的最佳出院策略仍不清楚。特别是,不应不加思考地恢复到住院前的用药。因此,患者和随访医生都应参与出院过程。在这项研究中,我们旨在测试一种简短的药物审查,该审查考虑了患者的优先事项,并结合了出院时的标准化沟通策略,是否会导致持续的药物适当性,并延长老年多病患者的再入院时间。
该研究设计为一项双臂、双盲、整群随机试验,涉及 42 名资深医院医生(HP)及其初级 HP 以及 2100 名 60 岁或以上的多病患者。使用随机最小化策略,资深 HP 将被分配到干预组或对照组。根据研究小组的指示,干预组的资深 HP 将指导其初级 HP 将一种简单的药物审查工具与定义的沟通策略结合起来,纳入病房的出院程序。对照组的未经培训的 HP 将提供关于常规护理的数据,他们的患者将按照当地的常规程序出院。主要结局是出院后 6 个月内再次入院的时间,次要结局包括再入院率、急诊和全科医生就诊次数、开处药物的种类和数量、潜在不适当药物的比例,以及患者出院后的生活质量。此外,还将在干预前收集 HP 和患者的特征。使用定性研究方法,将平行于正在进行的核心研究评估过程评估结果。
迄今为止,减少多种药物治疗的干预措施在 HP 和全科医生之间的关键接口仍然很少。据我们所知,这项试验是第一个分析在出院时和出院后早期使用简短的药物减停干预措施与标准化沟通策略相结合的试验。
ISRCTN,ISRCTN8427377。于 2018 年 1 月 11 日注册。