Institute for Response-Genetics, Department of Psychiatry, Psychotherapy and Psychosomatics, Psychiatric University Hospital, CH-8032, Zurich, Switzerland.
Department of Psychiatry, Psychotherapy, and Psychosomatics, University of Halle, D-06112, Halle, Germany.
Eur Arch Psychiatry Clin Neurosci. 2022 Jun;272(4):603-619. doi: 10.1007/s00406-021-01358-5. Epub 2021 Nov 25.
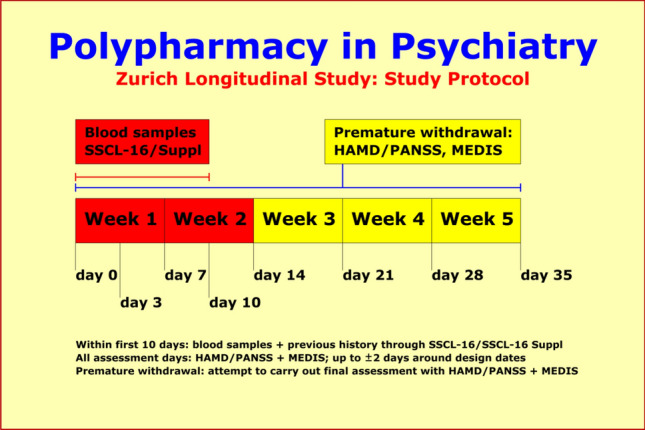
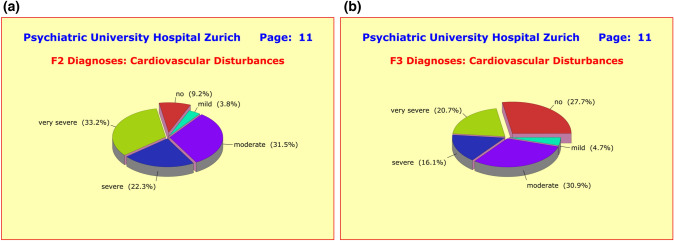
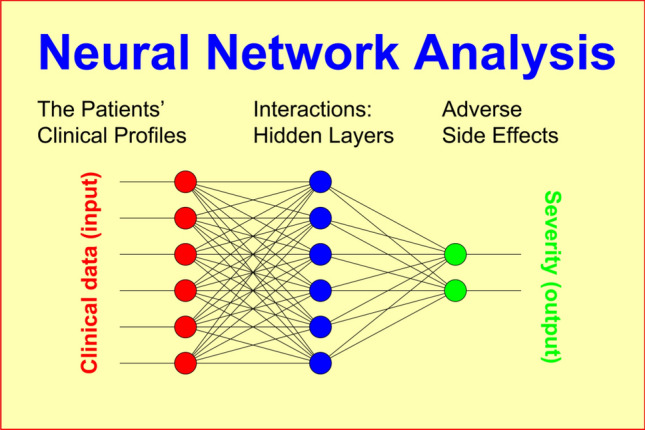
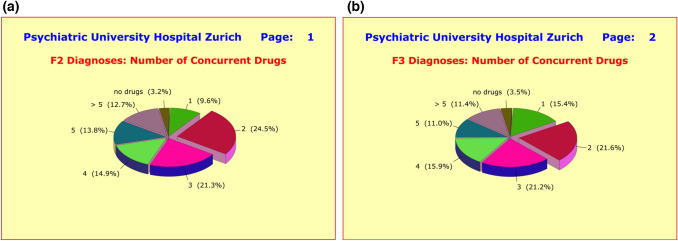
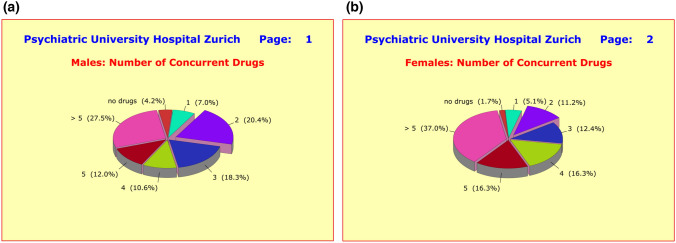
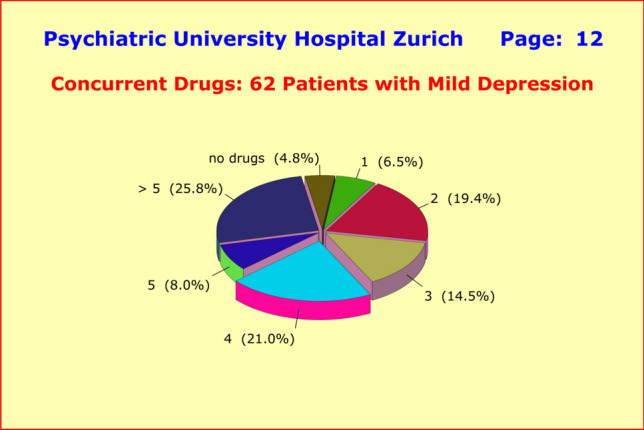
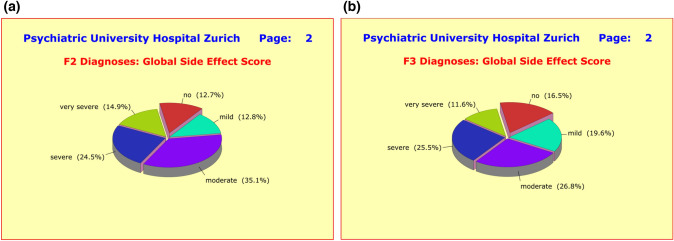
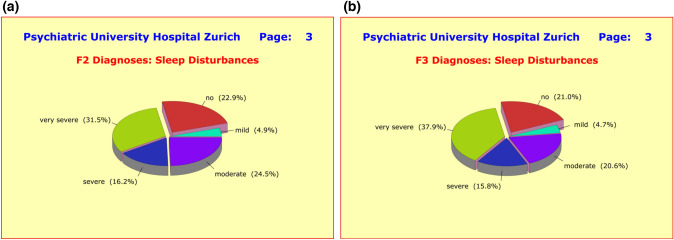
Current treatment standards in psychiatry are oriented towards polypharmacy, that is, patients receive combinations of several antidepressants, antipsychotics, mood stabilizers, anxiolytics, hypnotics, antihistamines, and anticholinergics, along with other somatic treatments. In tandem with the beneficial effects of psychopharmacological drug treatment, patients experience significant adverse reactions which appear to have become more frequent and more severe with the rise of ubiquitous polypharmacy. In this study, we aimed to assess today's acute inpatient treatment of depressive and schizophrenic disorders with focus on therapeutic strategies, medications, adverse side effects, time course of recovery, and efficacy of treatments. Of particular interest was the weighing of the benefits and drawbacks of polypharmacy regimens. We recruited a total of 320 patients hospitalized at three residential mental health treatment centers with a diagnosis of either schizophrenic (ICD-10: "F2x.x"; n = 94; "F2 patients") or depressive disorders (ICD-10: "F3x.x"; n = 226; "F3 patients"). The study protocol included (1) assessment of previous history by means of the SADS Syndrome Check List SSCL-16 (lifetime version); (2) repeated measurements over 5 weeks assessing the time course of improvement by the Hamilton Depression Scale HAM-D and the Positive and Negative Syndrome Scale PANSS, along with medications and adverse side effects through the Medication and Side Effects Inventory MEDIS; and (3) the collection of blood samples from which DNA and serum were extracted. Polypharmacy was by far the most common treatment regimen (85%) in this study. On average, patients received 4.50 ± 2.68 medications, consisting of 3.30 ± 1.84 psychotropic drugs, plus 0.79 ± 1.13 medications that alleviate adverse side effects, plus 0.41 ± 0.89 other somatic medications. The treating psychiatrists appeared to be the main determining factor in this context, while «previous history» and «severity at baseline» played a minor role, if at all. Adverse drug reactions were found to be an inherent component of polypharmacy and tended to have a 2-3 times higher incidence compared to monotherapy. Severe adverse reactions could not be attributed to a particular drug or drug combination. Rather, the empirical data suggested that severe side effects can be triggered by virtually all combinations of drugs, provided patients have a respective vulnerability. In terms of efficacy, there were no advantages of polypharmacy over monotherapy. The results of this study underlined the fact that polypharmacy regimens are not equally suited for every patient. Specifically, such regimens appeared to have a negative impact on treatment outcome and to obfuscate the "natural" time course of recovery through a multitude of interfering factors. Evidence clearly speaks against starting just every therapeutic intervention in psychiatry with a combination of psychopharmaceuticals. We think that it is time for psychiatry to reconsider its treatment strategies, which are far too one-sidedly fixated on psychopharmacology and pay far too little attention to alternative approaches, especially in mild cases where psychotherapy without concurrent medication should still be an option. Also, regular exercises and sports can definitely be an effective therapeutic means in a considerable number of cases. General practitioners (GPs) are particularly in demand here.
目前精神病学的治疗标准倾向于联合用药,即患者同时接受几种抗抑郁药、抗精神病药、心境稳定剂、抗焦虑药、催眠药、抗组胺药和抗胆碱能药物以及其他躯体治疗。随着精神药理学药物治疗的有益效果,患者出现了明显的不良反应,而且随着普遍联合用药的出现,这些不良反应似乎变得更加频繁和严重。在这项研究中,我们旨在评估目前抑郁症和精神分裂症的急性住院治疗,重点关注治疗策略、药物、不良反应、恢复时间和治疗效果。特别关注联合用药方案的利弊权衡。我们共招募了 320 名在三家住宅心理健康治疗中心住院的患者,他们的诊断为精神分裂症(ICD-10:“F2x.x”;n=94;“F2 患者”)或抑郁症(ICD-10:“F3x.x”;n=226;“F3 患者”)。研究方案包括:(1)通过 SADS 综合征检查表 SSCL-16(终身版)评估既往病史;(2)通过汉密尔顿抑郁量表 HAM-D 和阳性与阴性症状量表 PANSS 评估 5 周内的改善时间过程,以及通过药物和副作用清单 MEDIS 评估药物和副作用;(3)采集血液样本,从中提取 DNA 和血清。联合用药是该研究中最常见的治疗方案(85%)。平均而言,患者接受了 4.50±2.68 种药物,其中包括 3.30±1.84 种精神药物,加上 0.79±1.13 种缓解不良反应的药物,加上 0.41±0.89 种其他躯体药物。在这种情况下,主治精神科医生似乎是主要的决定因素,而“既往病史”和“基线严重程度”则几乎没有发挥作用,如果有的话。药物不良反应是联合用药的固有组成部分,与单药治疗相比,其发生率高出 2-3 倍。严重的不良反应不能归因于特定的药物或药物组合。相反,实证数据表明,严重的副作用几乎可以由所有药物组合引发,只要患者具有相应的易感性。在疗效方面,联合用药并不优于单药治疗。这项研究的结果强调了这样一个事实,即联合用药方案并不适合每个患者。具体而言,此类方案似乎对治疗结果产生了负面影响,并通过多种干扰因素模糊了“自然”的恢复时间过程。有证据明确反对在精神病学中每一次治疗干预都以联合使用精神药物开始。我们认为,精神病学应该重新考虑其治疗策略,这些策略过于片面地专注于精神药理学,而对替代方法关注太少,特别是在轻度病例中,不伴药物治疗的心理治疗仍然应该是一种选择。此外,定期锻炼和运动肯定可以成为相当多病例的有效治疗手段。全科医生(GP)在这里尤其受到需求。