Pisciotta Chiara, Saveri Paola, Pareyson Davide
Unit of Rare Neurodegenerative and Neurometabolic Diseases, Department of Clinical Neurosciences, Fondazione IRCCS Istituto Neurologico Carlo Besta, Via Celoria 11, 20133 Milan, Italy.
Brain Sci. 2021 Oct 29;11(11):1447. doi: 10.3390/brainsci11111447.
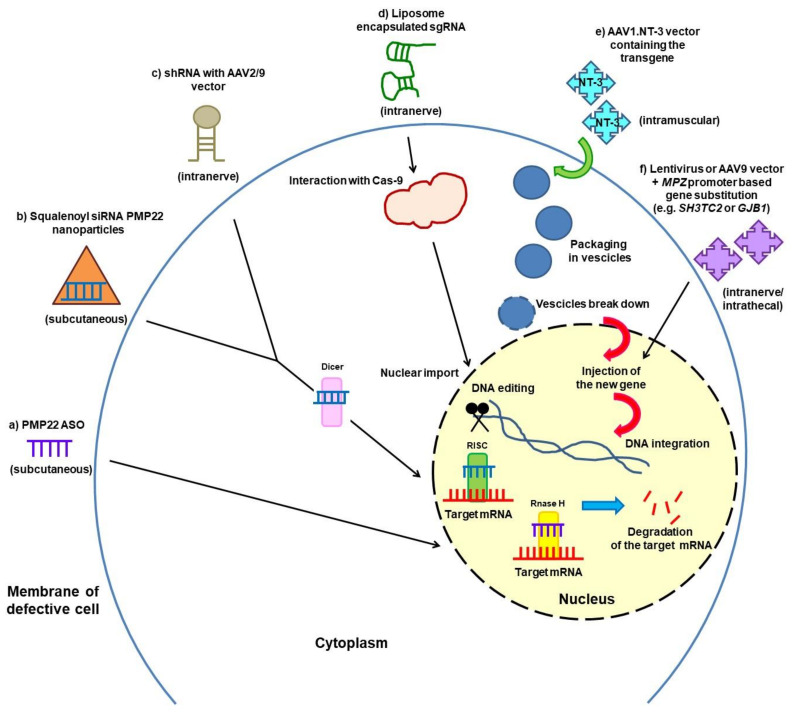
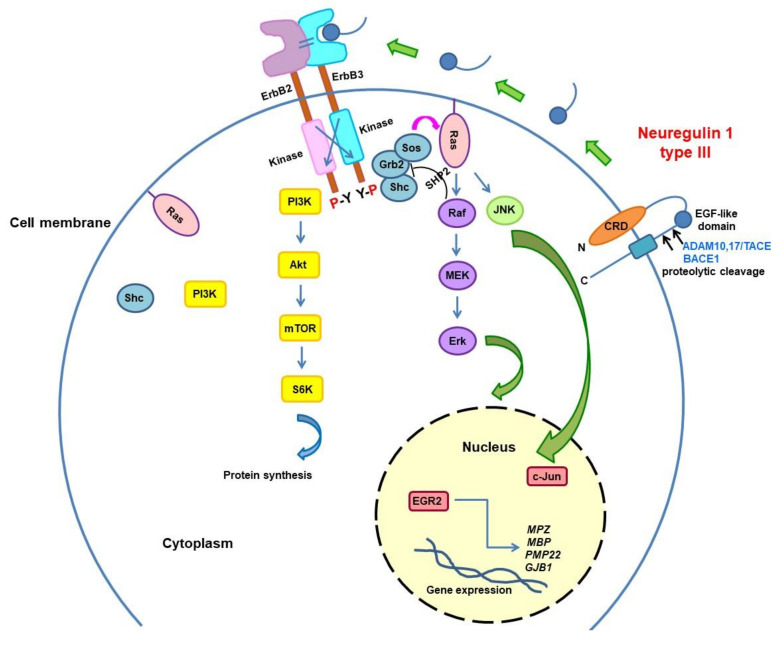
There is still no effective drug treatment available for Charcot-Marie-Tooth neuropathies (CMT). Current management relies on rehabilitation therapy, surgery for skeletal deformities, and symptomatic treatment of pain; fatigue and cramps are frequent complaints that are difficult to treat. The challenge is to find disease-modifying therapies. Several approaches, including gene silencing, to counteract the gene overexpression in the most frequent CMT1A type are under investigation. PXT3003 is the compound in the most advanced phase for CMT1A, as a second-phase III trial is ongoing. Gene therapy to substitute defective genes or insert novel ones and compounds acting on pathways important for different CMT types are being developed and tested in animal models. Modulation of the Neuregulin pathway determining myelin thickness is promising for both hypo-demyelinating and hypermyelinating neuropathies; intervention on Unfolded Protein Response seems effective for rescuing misfolded myelin proteins such as P0 in CMT1B. HDAC6 inhibitors improved axonal transport and ameliorated phenotypes in different CMT models. Other potential therapeutic strategies include targeting macrophages, lipid metabolism, and Nav1.8 sodium channel in demyelinating CMT and the P2X7 receptor, which regulates calcium influx into Schwann cells, in CMT1A. Further approaches are aimed at correcting metabolic abnormalities, including the accumulation of sorbitol caused by biallelic mutations in the sorbitol dehydrogenase () gene and of neurotoxic glycosphingolipids in HSN1.
目前仍没有可用于治疗夏科-马里-图思病(CMT)的有效药物。当前的治疗方法依赖于康复治疗、针对骨骼畸形的手术以及疼痛的对症治疗;疲劳和抽筋是常见且难以治疗的症状。面临的挑战是找到能够改变疾病进程的疗法。包括基因沉默在内的几种针对最常见的CMT1A型中基因过度表达的方法正在研究中。PXT3003是针对CMT1A处于最先进阶段的化合物,一项二期III期试验正在进行。正在动物模型中研发和测试用于替代缺陷基因或插入新基因的基因疗法以及作用于不同CMT类型重要通路的化合物。调节决定髓鞘厚度的神经调节蛋白通路对于脱髓鞘性和髓鞘增厚性神经病都有前景;针对未折叠蛋白反应的干预似乎对挽救CMT1B中错误折叠的髓鞘蛋白如P0有效。组蛋白去乙酰化酶6(HDAC6)抑制剂改善了不同CMT模型中的轴突运输并改善了表型。其他潜在的治疗策略包括针对脱髓鞘性CMT中的巨噬细胞、脂质代谢和Nav1.8钠通道以及CMT1A中调节钙流入雪旺细胞的P2X7受体。进一步的方法旨在纠正代谢异常,包括由山梨醇脱氢酶()基因双等位基因突变引起的山梨醇积累以及遗传性感觉神经病1型(HSN1)中神经毒性糖鞘脂的积累。