Tsai Ming-Hsien, Liou Hung-Hsiang, Huang Yen-Chun, Lee Tian-Shyug, Chen Mingchih, Fang Yu-Wei
Division of Nephrology, Department of Internal Medicine, Shin-Kong Wu Ho-Su Memorial Hospital, Taipei 11101, Taiwan.
Department of Medicine, Fu-Jen Catholic University School of Medicine, New Taipei City 242062, Taiwan.
Healthcare (Basel). 2021 Oct 31;9(11):1484. doi: 10.3390/healthcare9111484.
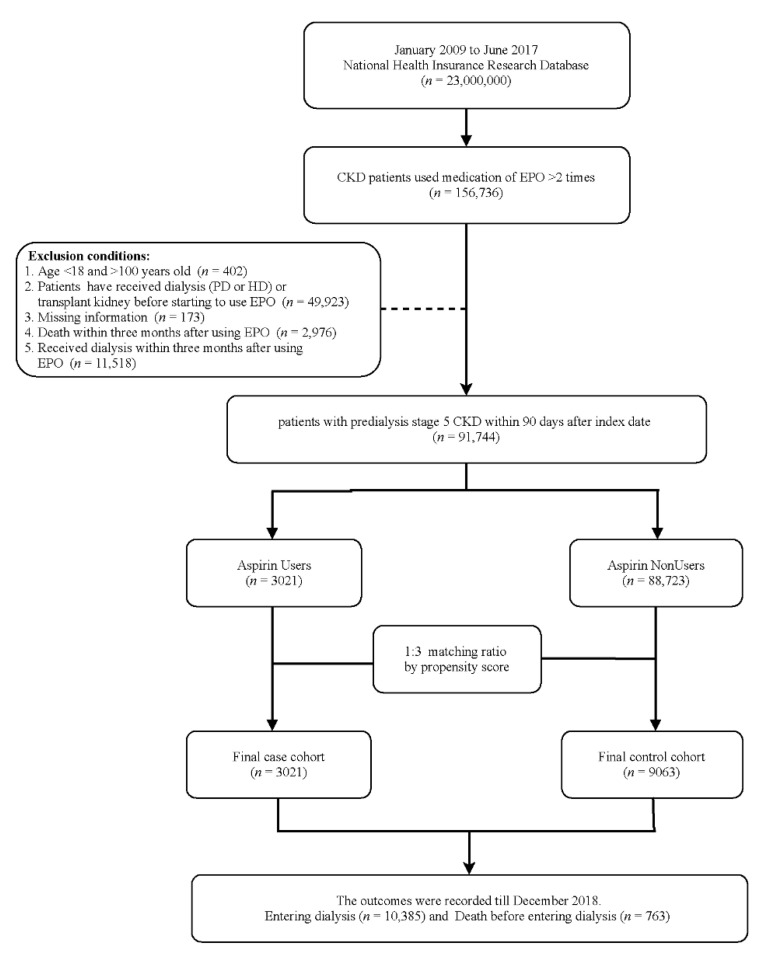
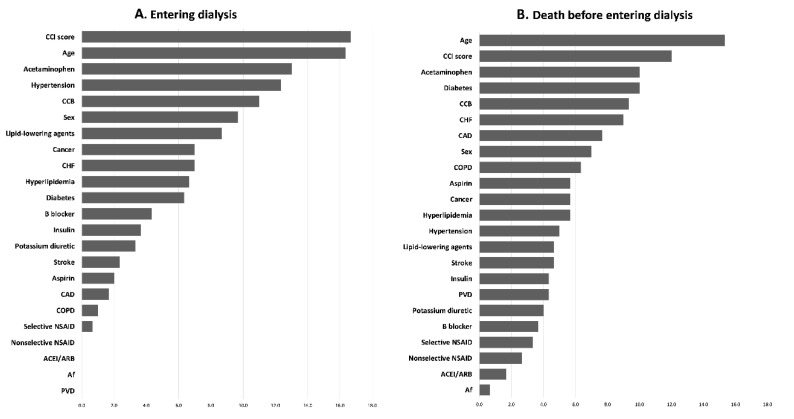
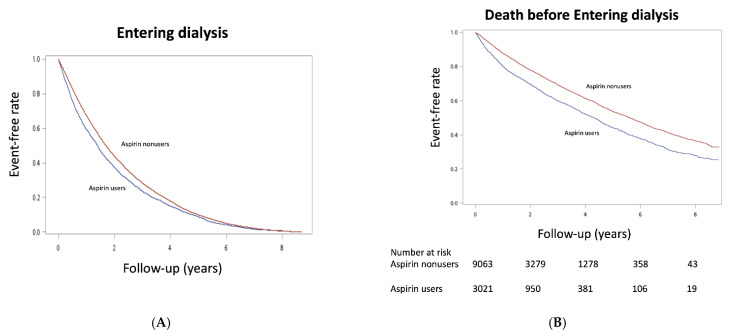
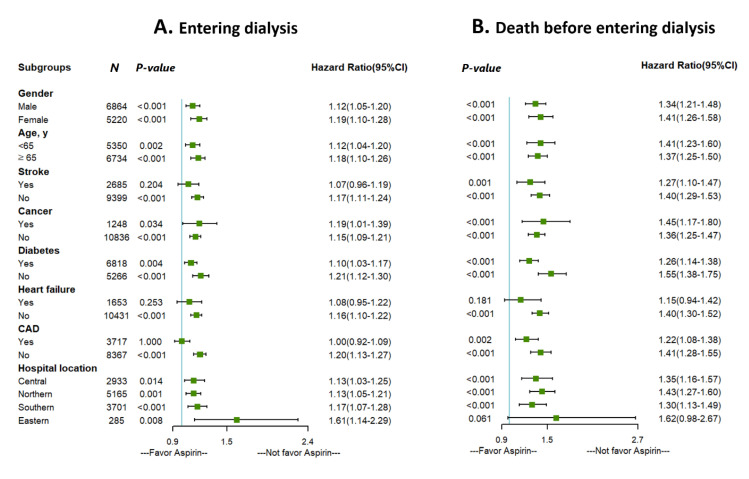
: Low-dose aspirin (100 mg) is widely used in preventing cardiovascular disease in chronic kidney disease (CKD) because its benefits outweighs the harm, however, its effect on clinical outcomes in patients with predialysis advanced CKD is still unclear. This study aimed to assess the effect of aspirin use on clinical outcomes in such group. : Patients were selected from a nationwide diabetes database from January 2009 to June 2017, and divided into two groups, a case group with aspirin use ( = 3021) and a control group without aspirin use ( = 9063), by propensity score matching with a 1:3 ratio. The Cox regression model was used to estimate the hazard ratio (HR). Moreover, machine learning method feature selection was used to assess the importance of parameters in the clinical outcomes. : In a mean follow-up of 1.54 years, aspirin use was associated with higher risk for entering dialysis (HR, 1.15 [95%CI, 1.10-1.21]) and death before entering dialysis (1.46 [1.25-1.71]), which were also supported by feature selection. The renal effect of aspirin use was consistent across patient subgroups. Nonusers and aspirin users did not show a significant difference, except for gastrointestinal bleeding (1.05 [0.96-1.15]), intracranial hemorrhage events (1.23 [0.98-1.55]), or ischemic stroke (1.15 [0.98-1.55]). : Patients with predialysis advanced CKD and anemia who received aspirin exhibited higher risk of entering dialysis and death before entering dialysis by 15% and 46%, respectively.
低剂量阿司匹林(100毫克)因其益处大于危害而被广泛用于预防慢性肾脏病(CKD)患者的心血管疾病,然而,其对透析前晚期CKD患者临床结局的影响仍不明确。本研究旨在评估使用阿司匹林对此类患者临床结局的影响。患者选自2009年1月至2017年6月的全国糖尿病数据库,并通过倾向得分1:3匹配分为两组,即使用阿司匹林的病例组(n = 3021)和未使用阿司匹林的对照组(n = 9063)。采用Cox回归模型估计风险比(HR)。此外,使用机器学习方法进行特征选择以评估临床结局中参数的重要性。在平均1.54年的随访中,使用阿司匹林与进入透析的较高风险(HR,1.15 [95%CI,1.10 - 1.21])和进入透析前死亡的较高风险(1.46 [1.25 - 1.71])相关,这也得到了特征选择的支持。使用阿司匹林的肾脏效应在各患者亚组中是一致的。除了胃肠道出血(1.05 [0.96 - 1.15])、颅内出血事件(1.23 [0.98 - 1.55])或缺血性卒中(1.15 [0.98 - 1.55])外,未使用者和阿司匹林使用者之间未显示出显著差异。透析前晚期CKD且贫血的患者使用阿司匹林后进入透析和进入透析前死亡的风险分别增加了15%和46%。