Jönköping Academy, Jönköping University, Box 1026, Jönköping 55111, Sweden.
Region Jönköping, Box 1024, Jönköping 55111, Sweden.
Int J Qual Health Care. 2021 Nov 29;33(Supplement_2):ii15-ii22. doi: 10.1093/intqhc/mzab060.
Pursuing the vision 'for a good life in an attractive region,' the Region Jönköping County (RJC) in Sweden oversees public health and health-care services for its 360 000 residents. For more than three decades, RJC has applied 'quality as strategy,' which has included increasing involvement of patients, family and friends and citizens. This practice has evolved, coinciding with the growing recognition of co-production as a fundamental feature in health-care services. This study views co-production as an umbrella term including different methods, initiatives and organizational levels. When learning about co-production in health-care services, it can be helpful to approach it as a dynamic and reflective process.
This study aims to describe the examples of key developmental steps toward co-production as a system property and to highlight 'lessons learned' from a Swedish health system's journey.
This qualitative descriptive study draws on interviews with key stakeholders and on documents, such as local policy documents, project reports, meeting protocols and presentations. Co-production initiatives were defined as strategies, projects, quality improvement (QI) programs or other efforts, which included persons with patient experience and/or their next of kin (PPE). We used directed manifest content analysis to identify initiatives, timelines and methods and inductive conventional content analysis to capture lessons learned over time.
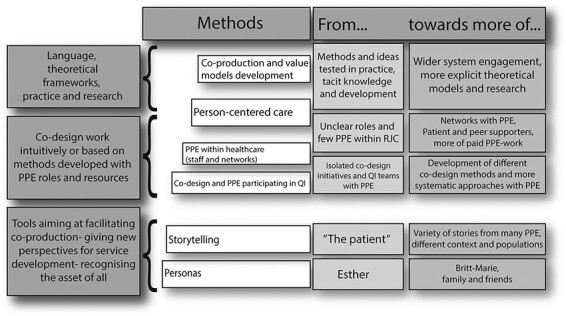
The directed content analyses identified 22 co-production initiatives from 1997 until today. Methods and approaches to facilitate co-production included development of personas, storytelling, person-centered care approaches, various co-design methods, QI interventions, harnessing of PPEs in different staff roles, and PPE-driven improvement and networks. The lessons learned included the following aspects of co-production: relations and structure; micro-, meso- and macro-level approaches; attitudes and roles; drivers for development; diversity; facilitating change; new perspectives on current work; consequences; uncertainties; theories and outcomes; and regulations and frames.
Co-production evolved as an increasingly significant aspect of services in the RJC health system. The initiatives examined in this study provide a broad overview and understanding of some of the RJC co-production journey, illustrating a health system's approach to co-production within a context of long-standing application of QI and microsystem theories. The main lessons include the constancy of direction, the strategy for improvement, engaged leaders, continuous learning and development from practical experience, and the importance of relationships with national and international experts in the pursuit of system-wide health-care co-production.
瑞典延雪平郡(RJC)追求“在有吸引力的地区享受美好生活”的愿景,负责其 36 万居民的公共卫生和医疗服务。三十多年来,RJC 一直应用“质量即战略”,这包括增加患者、家属和朋友以及公民的参与。这种做法随着共同生产作为医疗服务基本特征的认识不断提高而不断发展。本研究将共同生产视为一个包括不同方法、举措和组织层面的总称。在了解医疗服务中的共同生产时,将其视为一个动态和反思的过程可能会有所帮助。
本研究旨在描述将共同生产作为系统属性的关键发展步骤的实例,并突出展示瑞典卫生系统发展过程中的“经验教训”。
本定性描述性研究借鉴了对主要利益相关者的访谈以及当地政策文件、项目报告、会议协议和演示文稿等文件。共同生产举措被定义为包括具有患者体验和/或其近亲(PPE)的人员在内的战略、项目、质量改进(QI)计划或其他努力。我们使用定向显式内容分析来识别举措、时间表和方法,并使用归纳常规内容分析来捕获随着时间的推移而获得的经验教训。
定向内容分析从 1997 年至今确定了 22 项共同生产举措。促进共同生产的方法和方法包括开发角色模型、讲故事、以人为本的护理方法、各种共同设计方法、QI 干预、利用不同员工角色中的 PPE 以及 PPE 驱动的改进和网络。所获得的经验教训包括共同生产的以下方面:关系和结构;微观、中观和宏观层面的方法;态度和角色;发展动力;多样性;促进变革;对当前工作的新视角;后果;不确定性;理论和结果;以及法规和框架。
共同生产作为 RJC 卫生系统服务中越来越重要的方面不断发展。本研究中检查的举措提供了对 RJC 共同生产之旅的广泛概述和理解,说明了卫生系统在长期应用质量改进和微观系统理论的背景下对共同生产的方法。主要经验教训包括方向的恒定性、改进策略、积极参与的领导者、从实践经验中不断学习和发展,以及在追求全系统医疗保健共同生产方面与国内外专家建立关系的重要性。