Division of Cardiology, Department of Medical Biotechnologies, University of Siena, Viale Bracci 1, Siena, 53100, Italy.
Department of Thoracic and Cardiovascular Diseases, University of Eastern Piedmont, Maggiore della Carità Hospital, Novara, Italy.
ESC Heart Fail. 2022 Feb;9(1):476-485. doi: 10.1002/ehf2.13722. Epub 2021 Dec 7.
The present study investigated the prognostic impact of either isolated left atrial (LA) impairment, or its association with right ventricular (RV) failure, in heart failure (HF) with reduced ejection fraction (HFrEF), using basic and speckle tracking echocardiography (STE).
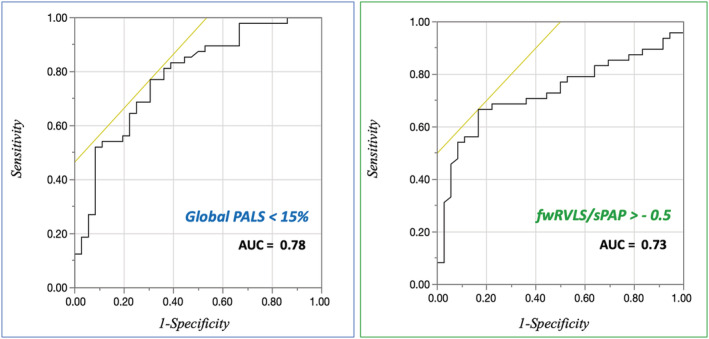
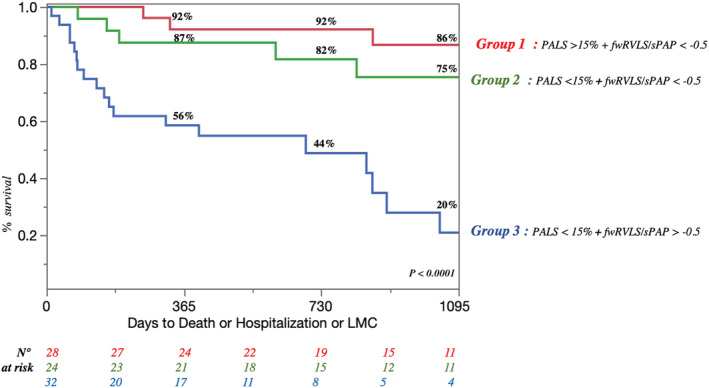
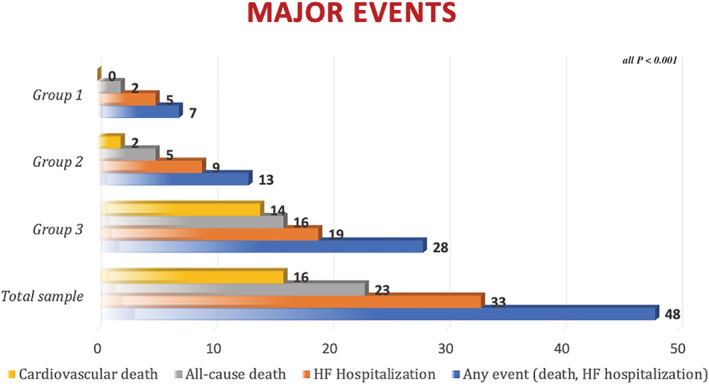
One hundred and six outpatients with HFrEF were enrolled in this prospective observational study. Patients with primary lung diseases, non-sinus rhythm, previous cardiac surgery, and poor acoustic window were excluded. After clinical examination and basic echocardiography, STE was used to measure peak atrial longitudinal strain (PALS) and a new marker of RV performance and pulmonary circulation relation: free-wall RV longitudinal strain (fwRVLS)/systolic pulmonary artery pressure (sPAP). Patients were followed for all-cause/cardiovascular death and HF hospitalization. Of 84 eligible patients (60.1 ± 11.5 years; 82% male patients), 48 reached the combined endpoint (cardiovascular death and/or HF hospitalization). Population was divided into three groups: Group 1 (PALS ≥ 15 and fwRVLS/sPAP ≤ -0.5), Group 2 (PALS ≤ 15 and fwRVLS/sPAP ≤ -0.5), and Group 3 (PALS ≤ 15 and fwRVLS/sPAP > -0.5). Mean follow up was 3.5 ± 0.3 years. The higher severity groups were associated with higher LA volume index (P < 0.0001), New York Heart Association class (P = 0.02), mitral regurgitation (P = 0.0004) and tricuspid regurgitation grades (P < 0.0001), lower left ventricular (LV) ejection fraction (P = 0.0003), LV global longitudinal strain (P < 0.0001), PALS (P < 0.0001), tricuspid annular plane systolic excursion (P < 0.007), sPAP (P < 0.0001), and RV strain (P < 0.0001). Reduced PALS and fwRVLS/sPAP were independent predictors of the combined endpoint with adjusted Cox models (hazard ratio = 9.54; 95% confidence interval = 2.95-30.92; P = 0.0002 for Group 3 vs. Group 1). Kaplan-Meier curves showed early and persistent divergence between the three groups for the prediction of the combined endpoint and of all-cause death (P < 0.0001).
The combination of LA and right heart damage entails worse prognosis in patients with HFrEF. The evaluation of PALS and fwRVLS/sPAP could aid risk stratification of HFrEF patients to provide them early treatment.
本研究旨在使用基础和斑点追踪超声心动图(STE),探讨孤立性左心房(LA)功能障碍或其与右心室(RV)衰竭的相关性对射血分数降低的心力衰竭(HFrEF)患者的预后影响。
本前瞻性观察性研究共纳入 106 例 HFrEF 门诊患者。排除了原发性肺部疾病、非窦性节律、既往心脏手术和超声心动图图像质量不佳的患者。在临床检查和基础超声心动图检查后,使用 STE 测量峰值心房纵向应变(PALS)和 RV 功能和肺循环关系的新标志物:游离壁 RV 纵向应变(fwRVLS)/收缩期肺动脉压(sPAP)。对所有患者进行全因/心血管死亡和 HF 住院的随访。在 84 名符合条件的患者(60.1±11.5 岁;82%为男性)中,有 48 名患者达到了联合终点(心血管死亡和/或 HF 住院)。将人群分为三组:组 1(PALS≥15 且 fwRVLS/sPAP≤-0.5)、组 2(PALS≤15 且 fwRVLS/sPAP≤-0.5)和组 3(PALS≤15 且 fwRVLS/sPAP>-0.5)。平均随访 3.5±0.3 年。严重程度较高的组与较高的左房容积指数(P<0.0001)、纽约心脏协会(NYHA)心功能分级(P=0.02)、二尖瓣反流(P=0.0004)和三尖瓣反流分级(P<0.0001)、较低的左心室(LV)射血分数(P=0.0003)、LV 整体纵向应变(P<0.0001)、PALS(P<0.0001)、三尖瓣环平面收缩期位移(P<0.007)、sPAP(P<0.0001)和 RV 应变(P<0.0001)相关。调整后的 Cox 模型显示,降低的 PALS 和 fwRVLS/sPAP 是联合终点的独立预测因素(危险比=9.54;95%置信区间=2.95-30.92;P=0.0002,组 3 与组 1 相比)。Kaplan-Meier 曲线显示,三组之间在预测联合终点和全因死亡方面存在早期和持续的差异(P<0.0001)。
LA 和右心损伤的组合对 HFrEF 患者的预后有更差的影响。评估 PALS 和 fwRVLS/sPAP 可以帮助 HFrEF 患者进行危险分层,以便早期进行治疗。