Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, BR.
Clinics (Sao Paulo). 2021 Dec 6;76:e3503. doi: 10.6061/clinics/2021/e3503. eCollection 2021.
To investigate the relationship between lung lesion burden (LLB) found on chest computed tomography (CT) and 30-day mortality in hospitalized patients with high clinical suspicion of coronavirus disease 2019 (COVID-19), accounting for tomographic dynamic changes.
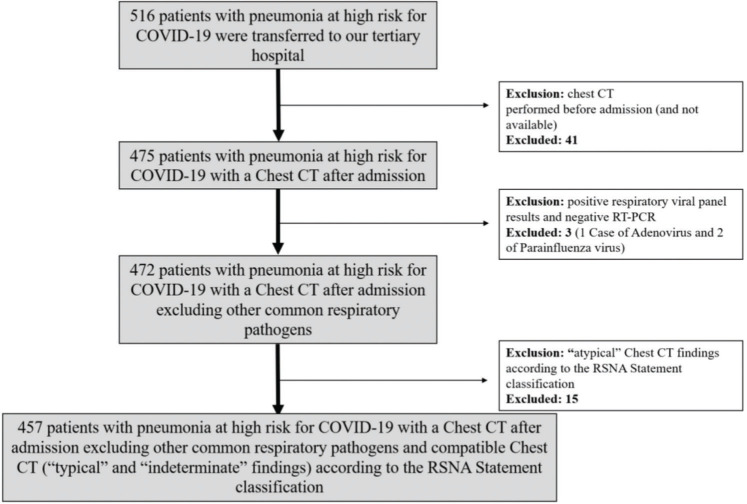
Patients hospitalized with high clinical suspicion of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in a dedicated and reference hospital for COVID-19, having undergone at least one RT-PCR test, regardless of the result, and with one CT compatible with COVID-19, were retrospectively studied. Clinical and laboratory data upon admission were assessed, and LLB found on CT was semi-quantitatively evaluated through visual analysis. The primary outcome was 30-day mortality after admission. Secondary outcomes, including the intensive care unit (ICU) admission, mechanical ventilation used, and length of stay (LOS), were assessed.
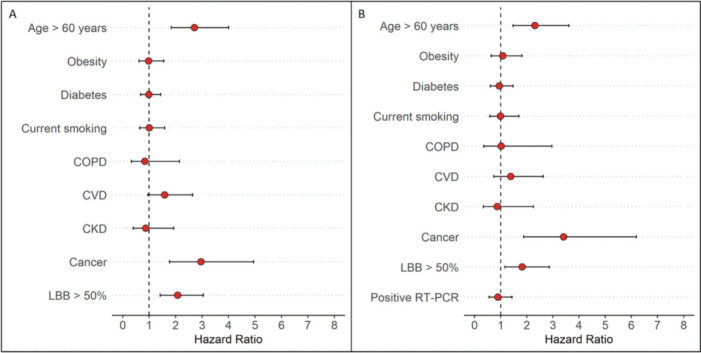
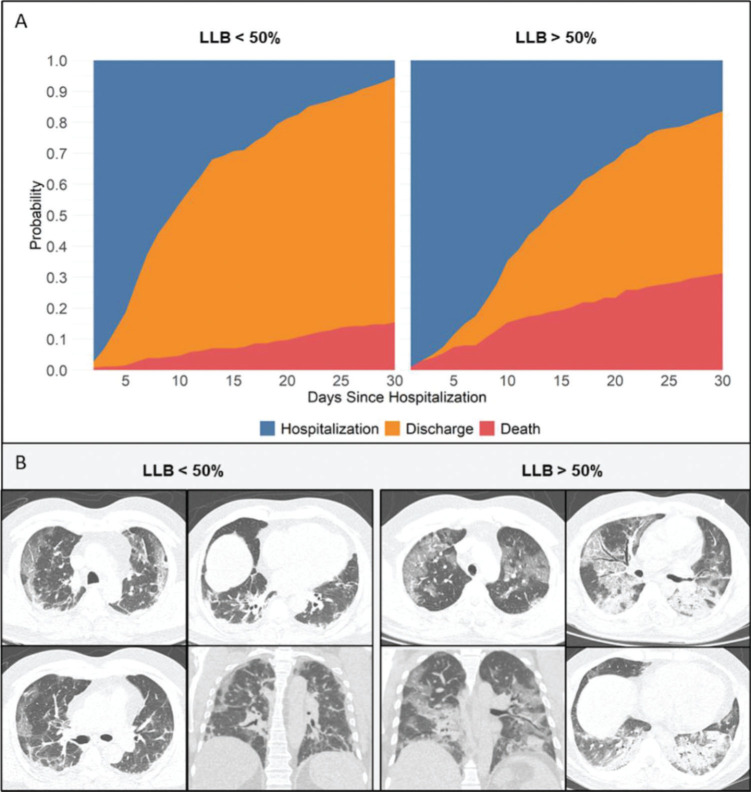
A total of 457 patients with a mean age of 57±15 years were included. Among these, 58% presented with positive RT-PCR result for COVID-19. The median time from symptom onset to RT-PCR was 8 days [interquartile range 6-11 days]. An initial LLB of ≥50% using CT was found in 201 patients (44%), which was associated with an increased crude at 30-day mortality (31% vs. 15% in patients with LLB of <50%, p<0.001). An LLB of ≥50% was also associated with an increase in the ICU admission, the need for mechanical ventilation, and a prolonged LOS after adjusting for baseline covariates and accounting for the CT findings as a time-varying covariate; hence, patients with an LLB of ≥50% remained at a higher risk at 30-day mortality (adjusted hazard ratio 2.17, 95% confidence interval 1.47-3.18, p<0.001).
Even after accounting for dynamic CT changes in patients with both clinical and imaging findings consistent with COVID-19, an LLB of ≥50% might be associated with a higher risk of mortality.
探讨胸部计算机断层扫描(CT)发现的肺部病变负担(LLB)与临床高度疑似 2019 年冠状病毒病(COVID-19)住院患者 30 天死亡率之间的关系,同时考虑到 CT 动态变化。
对一家专门的 COVID-19 参考医院中临床高度疑似严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染的住院患者进行回顾性研究,这些患者至少接受过一次 RT-PCR 检测,无论结果如何,且均有符合 COVID-19 的 CT 结果。评估入院时的临床和实验室数据,并通过视觉分析对 CT 上发现的 LLB 进行半定量评估。主要结局为入院后 30 天死亡率。次要结局包括入住重症监护病房(ICU)、使用机械通气和住院时间(LOS)。
共纳入 457 例平均年龄 57±15 岁的患者,其中 58%的患者 COVID-19 的 RT-PCR 结果为阳性。从症状出现到 RT-PCR 的中位时间为 8 天[四分位间距 6-11 天]。201 例(44%)患者 CT 上初始 LLB≥50%,粗死亡率为 31%,明显高于 LLB<50%的患者(15%,p<0.001)。调整基线协变量并将 CT 结果作为时变协变量后,LLB≥50%与 ICU 入住率、机械通气需求和 LOS 延长相关,因此,LLB≥50%的患者 30 天死亡率仍然更高(调整后的危险比 2.17,95%置信区间 1.47-3.18,p<0.001)。
即使考虑到符合 COVID-19 临床和影像学表现的患者 CT 动态变化,LLB≥50%也可能与更高的死亡率相关。