Department of Oncology, The First Affiliated Hospital of Anhui Medical University, 218 Jixi Road, Hefei, Anhui, 230022, People's Republic of China.
Department of Oncology, Ma'anshan Municipal People's Hospital, Ma'anshan, Anhui, 243000, People's Republic of China.
BMC Cancer. 2021 Dec 12;21(1):1326. doi: 10.1186/s12885-021-09079-7.
Survival times differ among patients with advanced gastric carcinoma. A precise and universal prognostic evaluation strategy has not yet been established. The current study aimed to construct a prognostic scoring model for mortality risk stratification in patients with advanced gastric carcinoma.
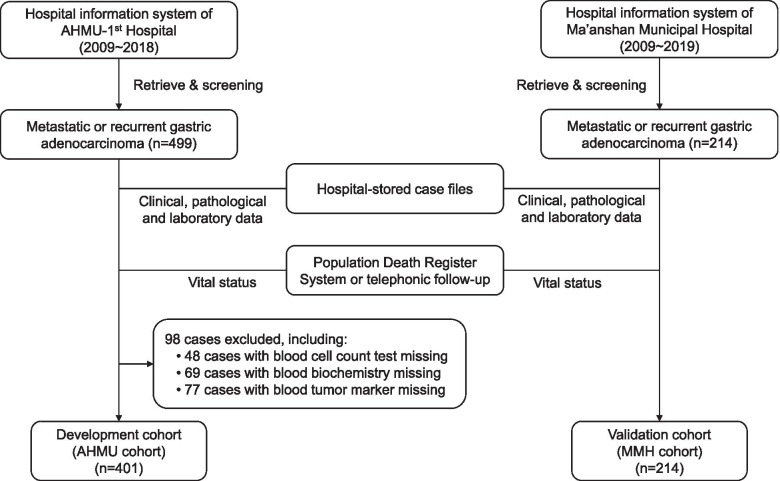
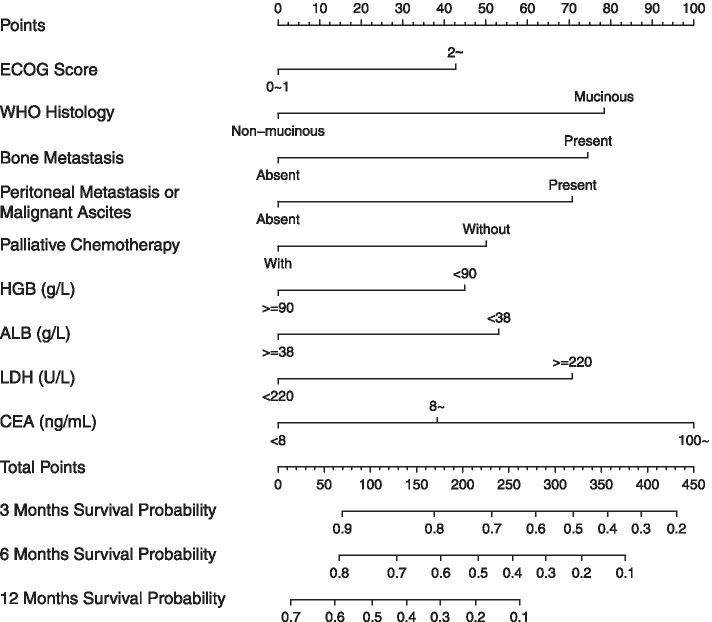
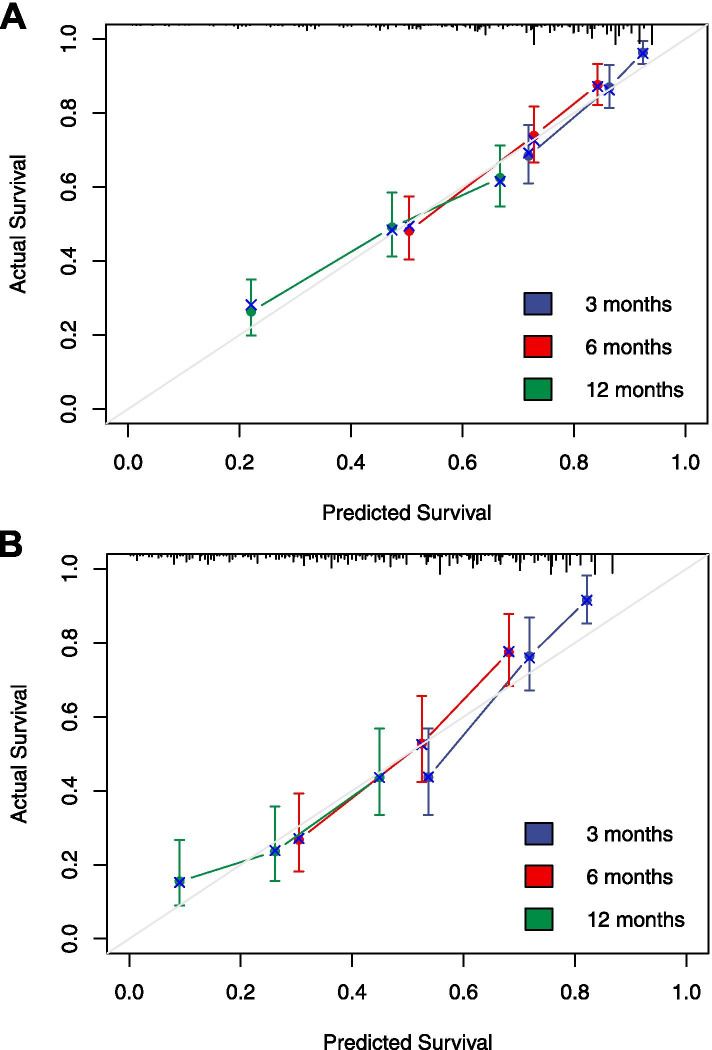
Patients with advanced gastric carcinoma from two hospitals (development and validation cohort) were included. Cox proportional hazards regression analysis was conducted to identify independent risk factors for survival. A prognostic nomogram model was developed using R statistics and validated both in bootstrap and external cohort. The concordance index and calibration curves were plotted to determine the discrimination and calibration of the model, respectively. The nomogram score and a simplified scoring system were developed to stratify patients in the two cohorts.
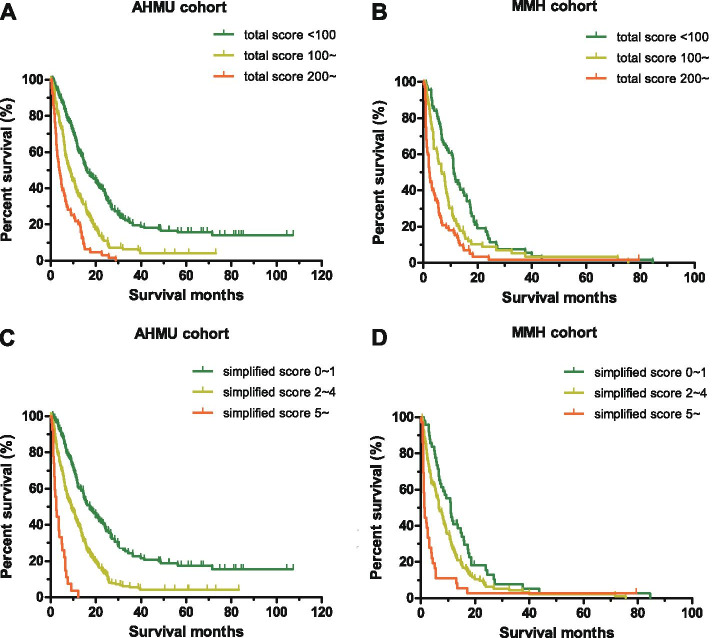
Development and validation cohort was comprised of 401 and 214 gastric cancer patients, respectively. Mucinous or non-mucinous histology, ECOG score, bone metastasis, ascites, hemoglobin concentration, serum albumin level, lactate dehydrogenase level, carcinoembryonic antigen level, and chemotherapy were finally incorporated into prognostic nomogram. The concordance indices were 0.689 (95% CI: 0.664 ~ 0.714) and 0.673 (95% CI: 0.632 ~ 0.714) for bootstrap and external validation. 100 and 200 were set as the cut-off values of nomogram score, patients in development cohort were stratified into low-, intermediate- and high-risk groups with median overall survival time 15.8 (95% CI: 12.2 ~ 19.5), 8.4 (95% CI: 6.7 ~ 10.2), and 3.9 (95% CI: 2.7 ~ 5.2) months, respectively; the cut-off values also worked well in validation cohort with different survival time in subgroups. A simplified model was also established and showed good consistency with the nomogram scoring model in both of development and validation cohorts.
The prognostic scoring model and its simplified surrogate can be used as tools for mortality risk stratification in patients with advanced gastric carcinoma.
晚期胃癌患者的生存时间存在差异。目前尚未建立精确且通用的预后评估策略。本研究旨在构建一种用于预测晚期胃癌患者死亡风险分层的预后评分模型。
纳入来自两家医院(开发和验证队列)的晚期胃癌患者。采用 Cox 比例风险回归分析确定生存的独立危险因素。使用 R 统计软件建立预后列线图模型,并在 bootstrap 和外部队列中进行验证。分别绘制一致性指数和校准曲线以确定模型的区分度和校准度。开发列线图评分和简化评分系统,以对两个队列中的患者进行分层。
开发和验证队列分别包含 401 例和 214 例胃癌患者。黏液或非黏液组织学、ECOG 评分、骨转移、腹水、血红蛋白浓度、血清白蛋白水平、乳酸脱氢酶水平、癌胚抗原水平和化疗最终被纳入预后列线图。bootstrap 和外部验证的一致性指数分别为 0.689(95%CI:0.6640.714)和 0.673(95%CI:0.6320.714)。将列线图评分设为 100 和 200 作为截断值,开发队列中的患者被分为低、中、高危组,中位总生存期分别为 15.8(95%CI:12.219.5)、8.4(95%CI:6.710.2)和 3.9(95%CI:2.7~5.2)个月;在验证队列中,不同生存时间的亚组也表现出良好的截断值。还建立了一个简化模型,在开发和验证队列中与列线图评分模型具有良好的一致性。
该预后评分模型及其简化替代模型可作为预测晚期胃癌患者死亡风险分层的工具。