Lee Hyunjung, Singh Gopal K
Oak Ridge Institute for Science and Education (ORISE), Oak Ridge, Tennessee, USA.
US Department of Health and Human Services, Health Resources and Services Administration, Office of Health Equity, Rockville, Maryland, USA.
Health Equity. 2021 Nov 9;5(1):770-779. doi: 10.1089/heq.2021.0036. eCollection 2021.
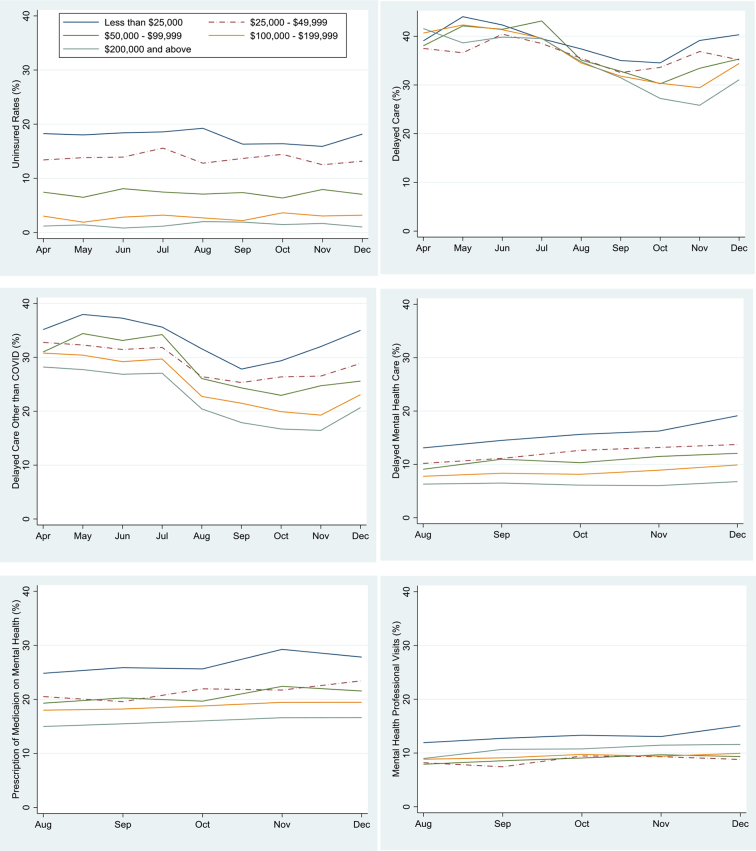
Since the start of the coronavirus disease 2019 (COVID-19) pandemic in March 2020, ∼40% of U.S. adults have experienced delayed medical care. Rates of uninsurance, delayed care, and utilization of mental health services during the course of the pandemic have not been analyzed in detail. We examined monthly trends and disparities in access to care by household income levels in the United States. Using Census Bureau's nationally representative pooled 2020 Household Pulse Survey from April to December, 2020 (=778,819), logistic regression models were used to analyze trends and inequalities in various access to care measures. During the COVID-19 pandemic, the odds of being uninsured, having a delayed medical care due to pandemic, delayed care of something other than COVID-19, or delayed mental health care were, respectively, 5.54, 1.50, 1.85, and 2.18 times higher for adults with income <$25,000, compared to those with incomes ≥$200,000, controlling for age, sex, race/ethnicity, education, marital status, housing tenure, region of residence, and survey month. Income inequities in mental health care widened over the course of the pandemic, while the probability of delayed mental health care increased for all income groups. Although the odds of taking prescription medication for mental health were higher for low-income adults, the odds of receiving mental health services were generally lower for lower income adults, controlling for all covariates. In light of our findings on persistent health care inequities during the pandemic, increased policy efforts are needed to improve access to care in low-income populations as an equitable COVID-19 recovery response.
自2020年3月新型冠状病毒肺炎(COVID-19)大流行开始以来,约40%的美国成年人经历了医疗护理延迟。在大流行期间,未参保率、护理延迟以及心理健康服务的利用率尚未得到详细分析。我们研究了美国按家庭收入水平划分的每月就医趋势和差异。利用美国人口普查局2020年4月至12月具有全国代表性的综合家庭脉搏调查(n = 778,819),采用逻辑回归模型分析各种就医措施的趋势和不平等情况。在COVID-19大流行期间,收入低于25,000美元的成年人未参保、因大流行导致医疗护理延迟、非COVID-19相关护理延迟或心理健康护理延迟的几率,分别是收入≥200,000美元成年人的5.54倍、1.50倍、1.85倍和2.18倍,同时对年龄、性别、种族/族裔、教育程度、婚姻状况、住房保有情况、居住地区和调查月份进行了控制。在大流行期间,心理健康护理方面的收入不平等有所扩大,而所有收入群体的心理健康护理延迟概率均有所增加。尽管低收入成年人服用心理健康处方药的几率较高,但在控制所有协变量的情况下,低收入成年人接受心理健康服务的几率总体较低。鉴于我们在大流行期间发现持续存在的医疗保健不平等现象,需要加大政策力度,作为公平的COVID-19恢复应对措施,改善低收入人群的就医机会。