Segarra Alfons, Del Carpio Jacqueline, Marco Maria Paz, Jatem Elias, Gonzalez Jorge, Chang Pamela, Ramos Natalia, de la Torre Judith, Prat Joana, Torres Maria J, Montoro Bruno, Ibarz Mercedes, Pico Silvia, Falcon Gloria, Canales Marina, Huertas Elisard, Romero Iñaki, Nieto Nacho
Department of Nephrology, Arnau de Vilanova University Hospital, Lleida, Spain.
Department of Nephrology, Vall d'Hebron University Hospital, Barcelona, Spain.
Clin Kidney J. 2021 May 19;14(12):2524-2533. doi: 10.1093/ckj/sfab094. eCollection 2021 Dec.
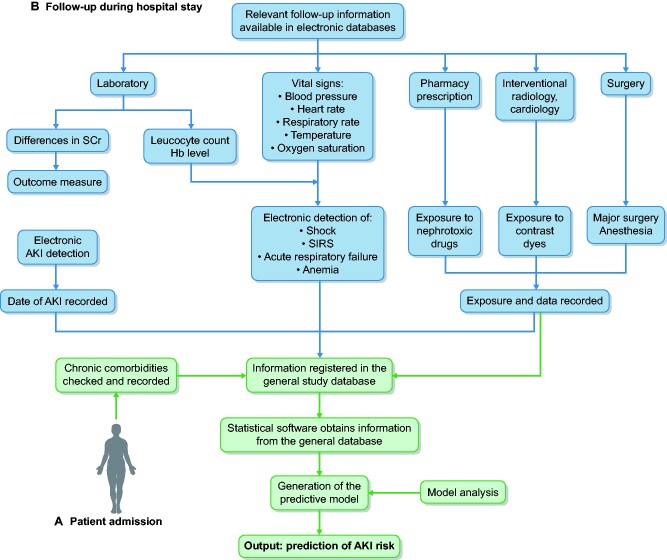
Models developed to predict hospital-acquired acute kidney injury (HA-AKI) in non-critically ill patients have a low sensitivity, do not include dynamic changes of risk factors and do not allow the establishment of a time relationship between exposure to risk factors and AKI. We developed and externally validated a predictive model of HA-AKI integrating electronic health databases and recording the exposure to risk factors prior to the detection of AKI.
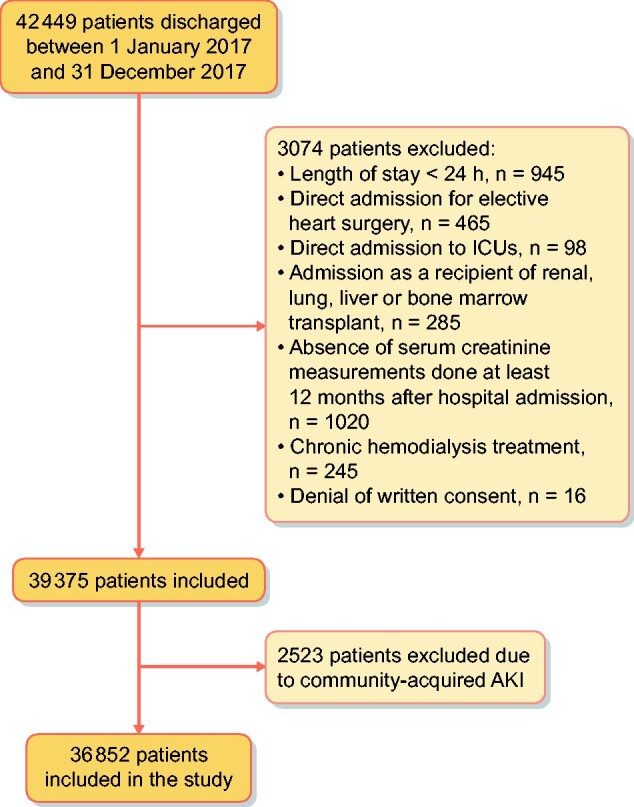
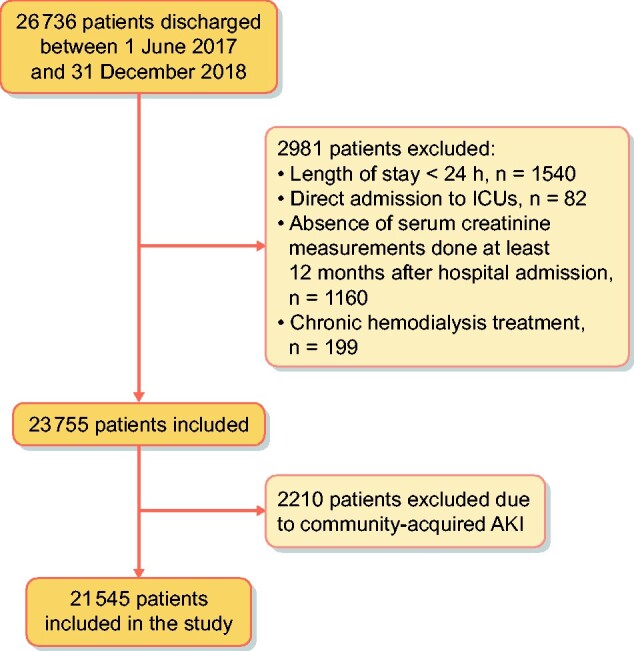
The study set was 36 852 non-critically ill hospitalized patients admitted from January to December 2017. Using stepwise logistic analyses, including demography, chronic comorbidities and exposure to risk factors prior to AKI detection, we developed a multivariate model to predict HA-AKI. This model was then externally validated in 21 545 non-critical patients admitted to the validation centre in the period from June 2017 to December 2018.
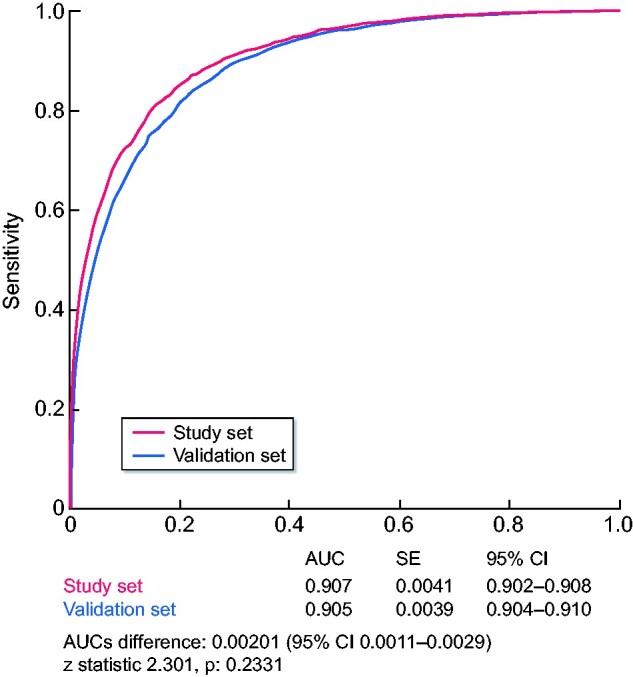
The incidence of AKI in the study set was 3.9%. Among chronic comorbidities, the highest odds ratios (ORs) were conferred by chronic kidney disease, urologic disease and liver disease. Among acute complications, the highest ORs were associated with acute respiratory failure, anaemia, systemic inflammatory response syndrome, circulatory shock and major surgery. The model showed an area under the curve (AUC) of 0.907 [95% confidence interval (CI) 0.902-0.908), a sensitivity of 82.7 (95% CI 80.7-84.6) and a specificity of 84.2 (95% CI 83.9-84.6) to predict HA-AKI, with an adequate goodness-of-fit for all risk categories (χ = 6.02, P = 0.64). In the validation set, the prevalence of AKI was 3.2%. The model showed an AUC of 0.905 (95% CI 0.904-0.910), a sensitivity of 81.2 (95% CI 79.2-83.1) and a specificity of 82.5 (95% CI 82.2-83) to predict HA-AKI and had an adequate goodness-of-fit for all risk categories (χ = 4.2, P = 0.83). An online tool (predaki.amalfianalytics.com) is available to calculate the risk of AKI in other hospital environments.
By using electronic health data records, our study provides a model that can be used in clinical practice to obtain an accurate dynamic and updated assessment of the individual risk of HA-AKI during the hospital admission period in non-critically ill patients.
为预测非危重症患者医院获得性急性肾损伤(HA-AKI)而开发的模型敏感性较低,未纳入风险因素的动态变化,且无法确定风险因素暴露与急性肾损伤之间的时间关系。我们开发并进行了外部验证了一个HA-AKI预测模型,该模型整合了电子健康数据库,并记录了急性肾损伤检测前的风险因素暴露情况。
研究队列包括2017年1月至12月收治的36852例非危重症住院患者。通过逐步逻辑分析,包括人口统计学、慢性合并症以及急性肾损伤检测前的风险因素暴露情况,我们开发了一个多变量模型来预测HA-AKI。然后,该模型在2017年6月至2018年12月期间入住验证中心的21545例非危重症患者中进行了外部验证。
研究队列中急性肾损伤的发生率为3.9%。在慢性合并症中,慢性肾病、泌尿系统疾病和肝脏疾病的优势比(OR)最高。在急性并发症中,急性呼吸衰竭、贫血、全身炎症反应综合征、循环性休克和大手术的OR最高。该模型预测HA-AKI的曲线下面积(AUC)为0.907[95%置信区间(CI)0.902-0.908],敏感性为82.7(95%CI 80.7-84.6),特异性为84.2(95%CI 83.9-84.6),对所有风险类别具有良好的拟合优度(χ = 6.02,P = 0.64)。在验证队列中,急性肾损伤的患病率为3.2%。该模型预测HA-AKI的AUC为0.905(95%CI 0.904-0.910),敏感性为81.2(95%CI 79.2-83.1),特异性为82.5(95%CI 82.2-83),对所有风险类别具有良好的拟合优度(χ = 4.2,P = 0.83)。可通过在线工具(predaki.amalfianalytics.com)计算其他医院环境中急性肾损伤的风险。
通过使用电子健康数据记录,我们研究提供了一个可用于临床实践的模型,以在非危重症患者住院期间获得对HA-AKI个体风险的准确动态和最新评估。