Research Unit, Polonia University, Czestochowa, Poland.
Provincial Emergency Medical Service Dispatcher, Warsaw, Poland.
Cardiol J. 2021;28(6):816-824. doi: 10.5603/CJ.a2021.0168.
The main purposes of this meta-analysis are to update the information about the impact of coronavirus disease 2019 (COVID-19) pandemic on outcomes of in-hospital cardiac arrest (IHCA) and to investigate the impact of being infected by by severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) on IHCA outcomes.
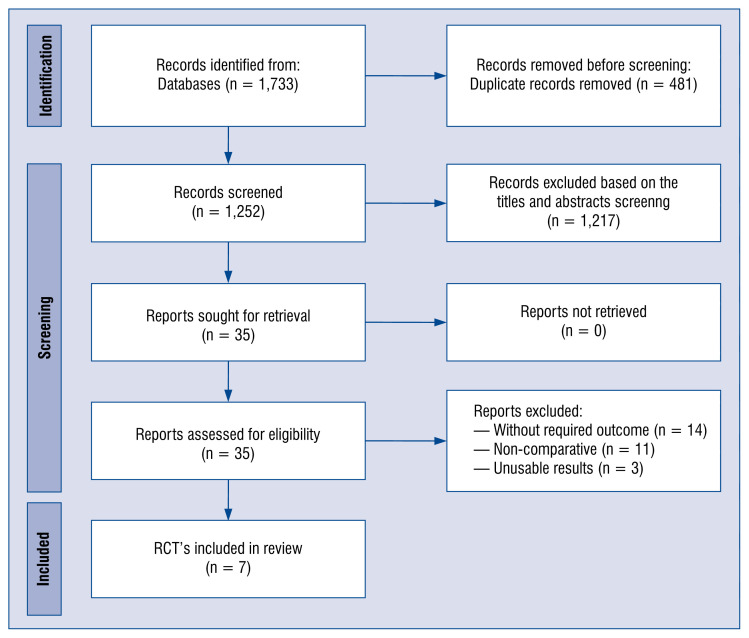
The current meta-analysis is an update and follows the recommendations of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
In analyses, pre- and intra-COVID-19 periods were observed for: shockable rhythms in 17.6% vs. 16.2% (odds ratio [OR]: 1.11; 95% confidence interval [CI]: 0.71-1.72; p = 0.65), return of spontaneous circulation (ROSC) in 47.4% vs. 44.0% (OR: 1.36; 95% CI: 0.90-2.07; p = 0.15), 30-day mortality in 59.8% vs. 60.9% (OR: 0.95; 95% CI: 0.75-1.22; p = 0.69) and overall mortality 75.8% vs. 74.7% (OR: 0.80; 95% CI: 0.49-1.28; p = 0.35), respectively. In analyses, SARS-CoV-2 positive and negative patients were observed for: shockable rhythms in 9.6% vs. 19.8% (OR: 0.51; 95% CI: 0.35-0.73; p < 0.001), ROSC in 33.9% vs. 52.1% (OR: 0.47; 95% CI: 0.30-0.73; p < 0.001), 30-day mortality in 77.2% vs. 59.7% (OR: 2.08; 95% CI: 1.28-3.38; p = 0.003) and overall mortality in 94.9% vs. 76.7% (OR: 3.20; 95% CI: 0.98-10.49; p = 0.05), respectively.
Despite ROSC, 30-day and overall mortality rate were not statistically different in pre- vs. intra-COVID-19 periods, a lower incidence of ROSC and higher 20-day mortality rate were observed in SARS-CoV-2 (+) compared to SARS-CoV-2 (-) patients.
本次荟萃分析的主要目的是更新关于 2019 年冠状病毒病(COVID-19)大流行对院内心脏骤停(IHCA)结局影响的信息,并探讨感染严重急性呼吸综合征冠状病毒 2 型(SARS-CoV-2)对 IHCA 结局的影响。
本次荟萃分析是对先前研究的更新,遵循系统评价和荟萃分析的首选报告项目(PRISMA)的建议。
在分析中,观察到 COVID-19 前和 COVID-19 期间:可除颤节律分别为 17.6%比 16.2%(比值比[OR]:1.11;95%置信区间[CI]:0.71-1.72;p=0.65)、自主循环恢复(ROSC)分别为 47.4%比 44.0%(OR:1.36;95%CI:0.90-2.07;p=0.15)、30 天死亡率分别为 59.8%比 60.9%(OR:0.95;95%CI:0.75-1.22;p=0.69)和总死亡率分别为 75.8%比 74.7%(OR:0.80;95%CI:0.49-1.28;p=0.35)。在分析中,观察到 SARS-CoV-2 阳性和阴性患者:可除颤节律分别为 9.6%比 19.8%(OR:0.51;95%CI:0.35-0.73;p<0.001)、ROSC 分别为 33.9%比 52.1%(OR:0.47;95%CI:0.30-0.73;p<0.001)、30 天死亡率分别为 77.2%比 59.7%(OR:2.08;95%CI:1.28-3.38;p=0.003)和总死亡率分别为 94.9%比 76.7%(OR:3.20;95%CI:0.98-10.49;p=0.05)。
尽管 ROSC,但 COVID-19 前与 COVID-19 期间的 30 天和总死亡率无统计学差异,与 SARS-CoV-2(-)患者相比,SARS-CoV-2(+)患者的 ROSC 发生率较低,20 天死亡率较高。