Department of Surgical, Oncological and Oral Science (Di.Chir.On.S.), University of Palermo, Italy.
Department of Surgical, Oncological and Oral Science (Di.Chir.On.S.), University of Palermo, Italy; Department of Anaesthesia, Intensive Care and Emergency, Policlinico Paolo Giaccone, Palermo, Italy.
Resuscitation. 2021 Jul;164:122-129. doi: 10.1016/j.resuscitation.2021.04.025. Epub 2021 May 5.
To estimate the mortality rate, the rate of return of spontaneous circulation (ROSC) and survival with favorable neurological outcome in patients with COVID-19 after in-hospital cardiac arrest (IHCA) and attempted cardiopulmonary resuscitation (CPR).
PubMed, EMBASE, Web of Science, bioRxiv and medRxiv were surveyed up to 8th February 2021 for studies reporting data on mortality of patients with COVID-19 after IHCA. The primary outcome sought was mortality (in-hospital or at 30 days) after IHCA with attempted CPR. Additional outcomes were the overall rate of IHCA, the rate of non-shockable presenting rhythms, the rate of ROSC and the rate of survival with favorable neurological status.
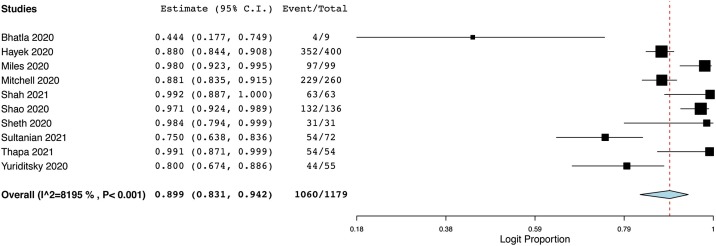
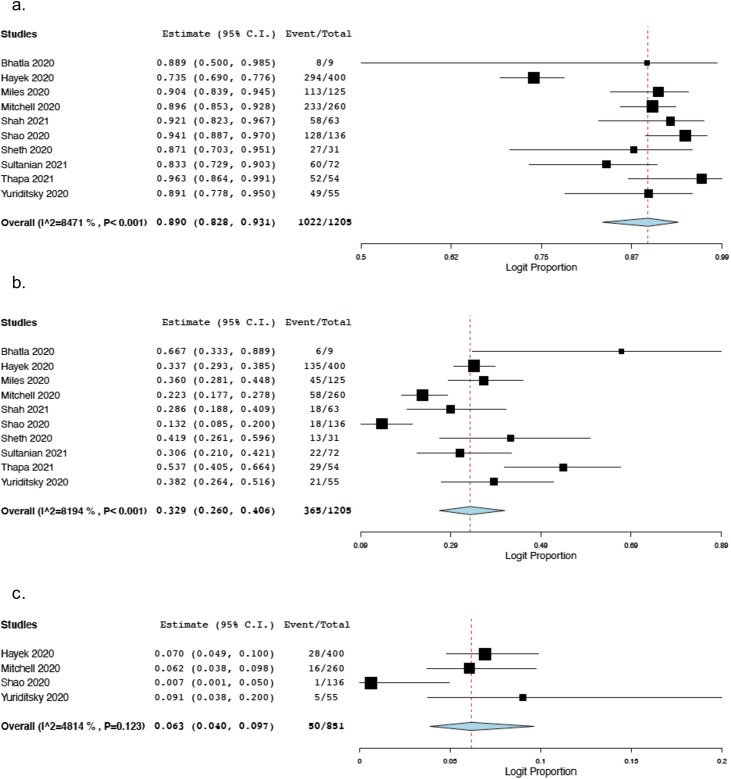
Ten articles were included in the systematic review and meta-analysis, for a total of 1179 COVID-19 patients after IHCA with attempted CPR. The estimated overall mortality rate (in-hospital or at 30 days) was 89.9% (95% Predicted Interval [P.I.] 83.1%-94.2%; 1060/1179 patients; I = 82%). The estimated rate of non-shockable presenting rhythms was 89% (95% P.I. 82.8%-93.1%; 1022/1205 patients; I = 85%), and the estimated rate of ROSC was 32.9% (95% P.I. 26%-40.6%; 365/1205 patients; I = 82%). The estimated overall rate of survival with favorable neurological status at 30 days was 6.3% (95% P.I. 4%-9.7%; 50/851 patients; I = 48%). Sensitivity analysis showed that COVID-19 patients had higher risk of death after IHCA than non COVID-19 patients (OR 2.34; 95% C.I. 1.37-3.99; number of studies = 3; 1215 patients).
Although one of three COVID-19 patients undergoing IHCA may achieve ROSC, almost 90% may not survive at 30 days or to hospital discharge.
评估 COVID-19 患者院内心搏骤停(IHCA)并尝试心肺复苏(CPR)后的死亡率、自主循环恢复(ROSC)率和神经功能良好的存活率。
检索 PubMed、EMBASE、Web of Science、bioRxiv 和 medRxiv,截至 2021 年 2 月 8 日,以获取报告 COVID-19 患者 IHCA 后死亡率数据的研究。主要结局是 IHCA 后尝试 CPR 的患者的院内或 30 天死亡率。其他结局包括 IHCA 的总体发生率、无除颤性初始节律的发生率、ROSC 率和神经功能良好的存活率。
10 篇文章被纳入系统评价和荟萃分析,共纳入 1179 例 COVID-19 患者 IHCA 后尝试 CPR。估计的总体死亡率(院内或 30 天)为 89.9%(95%预测区间[PI] 83.1%-94.2%;1060/1179 例患者;I = 82%)。估计的无除颤性初始节律率为 89%(95%PI 82.8%-93.1%;1022/1205 例患者;I = 85%),估计的 ROSC 率为 32.9%(95%PI 26%-40.6%;365/1205 例患者;I = 82%)。估计的 30 天神经功能良好的总体存活率为 6.3%(95%PI 4%-9.7%;50/851 例患者;I = 48%)。敏感性分析显示,COVID-19 患者 IHCA 后死亡风险高于非 COVID-19 患者(OR 2.34;95%CI 1.37-3.99;研究数量=3;1215 例患者)。
尽管 COVID-19 患者中有三分之一可能在 IHCA 后实现 ROSC,但近 90%的患者可能无法在 30 天或出院时存活。