Infectious Diseases Service, University Hospital and University of Lausanne, Lausanne, Switzerland.
Tropical Disease Unit, Department of Medicine, Sandra Rotman Centre for Global Health, University Health Network-Toronto General Hospital, University of Toronto, Toronto, Canada.
BMC Infect Dis. 2022 Jan 6;22(1):39. doi: 10.1186/s12879-021-06994-9.
Inappropriate antibiotics use in lower respiratory tract infections (LRTI) is a major contributor to resistance. We aimed to design an algorithm based on clinical signs and host biomarkers to identify bacterial community-acquired pneumonia (CAP) among patients with LRTI.
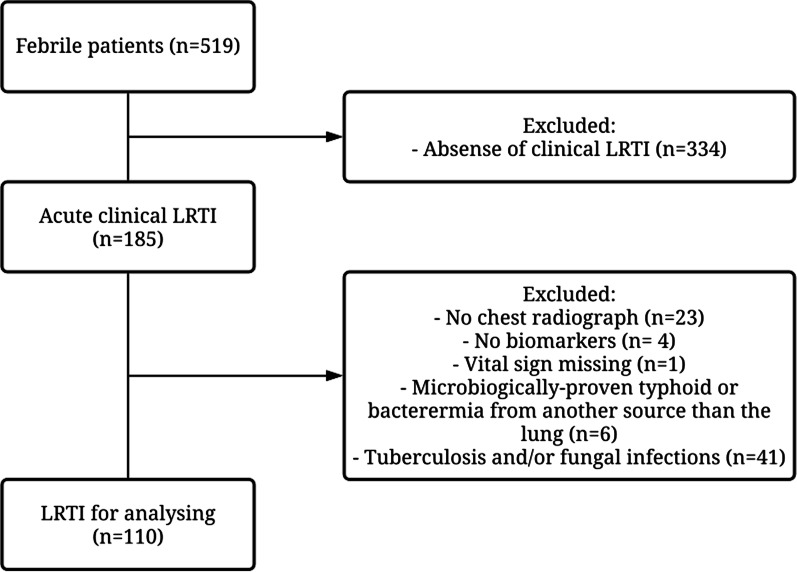
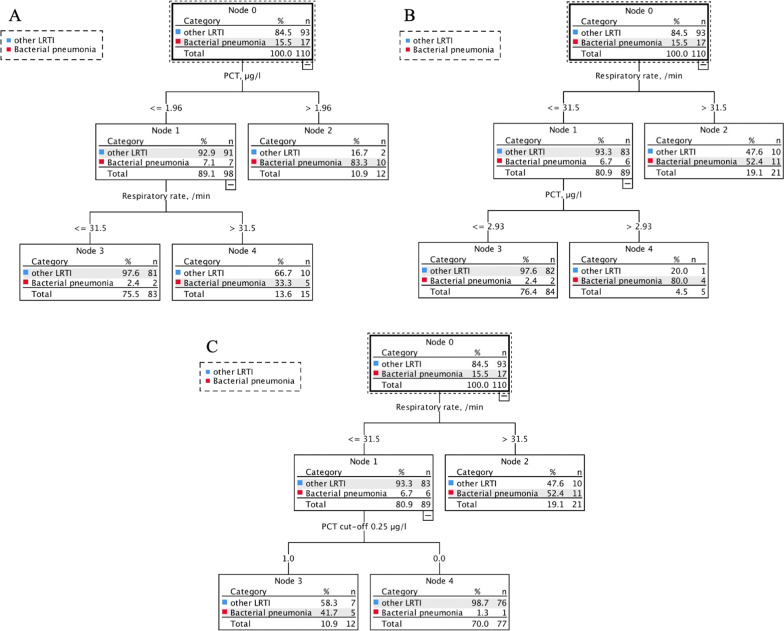
Participants with LRTI were selected in a prospective cohort of febrile (≥ 38 °C) adults presenting to outpatient clinics in Dar es Salaam. Participants underwent chest X-ray, multiplex PCR for respiratory pathogens, and measurements of 13 biomarkers. We evaluated the predictive accuracy of clinical signs and biomarkers using logistic regression and classification and regression tree analysis.
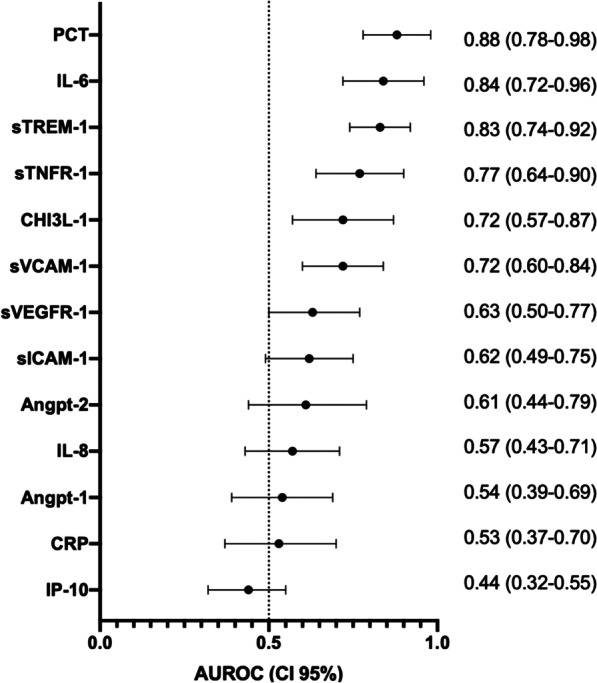
Of 110 patients with LRTI, 17 had bacterial CAP. Procalcitonin (PCT), interleukin-6 (IL-6) and soluble triggering receptor expressed by myeloid cells-1 (sTREM-1) showed an excellent predictive accuracy to identify bacterial CAP (AUROC 0.88, 95%CI 0.78-0.98; 0.84, 0.72-0.99; 0.83, 0.74-0.92, respectively). Combining respiratory rate with PCT or IL-6 significantly improved the model compared to respiratory rate alone (p = 0.006, p = 0.033, respectively). An algorithm with respiratory rate (≥ 32/min) and PCT (≥ 0.25 μg/L) had 94% sensitivity and 82% specificity.
PCT, IL-6 and sTREM-1 had an excellent predictive accuracy in differentiating bacterial CAP from other LRTIs. An algorithm combining respiratory rate and PCT displayed even better performance in this sub-Sahara African setting.
下呼吸道感染(LRTI)中抗生素的不适当使用是导致耐药的主要因素。我们旨在设计一种基于临床症状和宿主生物标志物的算法,以识别患有 LRTI 的细菌性社区获得性肺炎(CAP)患者。
在达累斯萨拉姆门诊发热(≥38°C)成人的前瞻性队列研究中选择患有 LRTI 的参与者。参与者接受胸部 X 光检查、呼吸道病原体多重 PCR 检查和 13 种生物标志物的测量。我们使用逻辑回归和分类回归树分析评估临床症状和生物标志物的预测准确性。
在 110 例 LRTI 患者中,有 17 例患有细菌性 CAP。降钙素原(PCT)、白细胞介素-6(IL-6)和可溶性髓系细胞触发受体-1(sTREM-1)均显示出出色的预测准确性,可识别细菌性 CAP(AUROC 0.88,95%CI 0.78-0.98;0.84,0.72-0.99;0.83,0.74-0.92,分别)。与单独使用呼吸频率相比,将呼吸频率与 PCT 或 IL-6 结合使用可显著改善模型(p=0.006,p=0.033)。呼吸频率(≥32/min)和 PCT(≥0.25μg/L)的算法具有 94%的敏感性和 82%的特异性。
PCT、IL-6 和 sTREM-1 在区分细菌性 CAP 与其他 LRTIs 方面具有出色的预测准确性。在撒哈拉以南非洲地区,将呼吸频率与 PCT 结合使用的算法具有更好的性能。